Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Rikshospitalet University Hospital
Division of Clinical Neuroscience Dept of Neuropsychiatry and Psychosomatic Medicine

2
Somatoform disorders Neurobiology

3
Somatisering Somatisk utredning Etiologi (teori)
Oversett somatisk sykdom Kommunikasjon Stress Hjernedysfunksjon Genetisk defekt Psykiatri Betinging Nevrobiologisk forskning Somatisk utredning alexithymi affektregulering-personlighet nevro……. molekylærbiologi biologisk psykiatri personlighet

4
Misdiagnosis of conversion symptoms and hysteria (mean %, 95% confidence
ntervals, random effects) plotted at midpoint of five year intervals according to when patients were diagnosed. Size of each point is proportional to number of subjects at each time point (total n=1466) (Stone et al, BMJ 2005;331:989)
 plotted at midpoint of five year intervals according to. when patients were diagnosed. Size of each point is proportional to number. of subjects at each time point (total n=1466) (Stone et al, BMJ 2005;331:989)")
6
Sammenhengen hjerne-kropp-stress Indre /ytre Psykiske symptomer stress
Adferdsendringer Nevroendokrine effekter CRF ACTH Nevrotransmittere Immunsystemet 5HT, DA, NA etc Cytokiner etc Nevropeptider Perifert blod: cytokiner, NK celle aktivitet Sammenhengen hjerne-kropp-stress Fra: Brigitta Bondy, MD Uni München Dialogues Clin Neurosci. 2003;5: Binyrer: kortisol, nor- adrenalin, adr. Hjertesymptomatologi Smerte Mage-tarm symptomatologi etc

7
CNS DISEASE Brain Immune response Neurological Manifestations
Chemical cascade Neuropeptides Cytokine balance + IL-1, IL-6, TNF - IL-1Ra, IL-4, IL-10, TGF Cytokines Neurotransmitters Neuroinflammation -neurotoxicity -neurodegeneration Signals PERIPHERAL DISEASE Plata-Salamán & Turin. Molecular Psychiatry 1999; 4: 302-6

8
Autoimmune diseases with higher lifetime prevalence among
schizophrenia patients than among comparison subjects at a 95% level of statistical significance (Danish register data) Eaton et al. American Journal of Psychiatry 163: , March 2006 thyrotoxicosis, intestinal malabsorption, acquired hemolytic anemia, chronic active hepatitis, interstitial cystitis, alopecia areata, myositis, polymyalgia rheumatica, Sjögren’s syndrome
 Eaton et al. American Journal of Psychiatry 163: , March thyrotoxicosis, intestinal malabsorption, acquired hemolytic anemia, chronic active hepatitis, interstitial cystitis, alopecia areata, myositis, polymyalgia rheumatica, Sjögren’s syndrome.")
9
Increased expression of class II antigens
Hassan et al. Dep of Infect and Trop. Diseases, Royal Freee, London 2001: Increased expression of class II antigens Reduced expression of costimulatory receptor CD28 (marker of terminally differentiated cells) lends support to the concept of immunoactivation of T-lymphocytes in CFS and consistent with a viral etiopahtogenesis
 lends support to the concept of immunoactivation of. T-lymphocytes in CFS. and. consistent with a viral etiopahtogenesis.")
10
Virus infection and CFS
Virus may provoke CFS Unclear pathophysiology (infection? Immune response? Other factors?) Important: The majority do not develop CFS after virus infections I.e. Non-infectious aspects must be of important for outcome, but may not explain all variance in CFS cases
 Important: The majority do not develop CFS after virus infections. I.e. Non-infectious aspects must be of important for outcome, but may not explain all variance in CFS cases.")
11
”Briquets syndrom” Schizofreni frontale forandringer +
temporale forandringer dysfunksjon dominante hemisfære etc patologi ERP Briquets syndrom frontale forandringer Ikke-dominant hemisfære dominerer patologi ERP

12
Hjernedysfunksjon og Briquet?
bifrontal svekkelse i hemisfærefunksjoner dominans av ikke-dominante hemisfære patologisk evoked potentials I motsetning til raske pasienter: reagerer likt på relevante OG ikke-relevante stimuli (?)
")
13
Genetikk og Briquets syndrom?
Kvinner multiple somatiske symptomer og uakseptabel adferd: somatiseringslidelse Menn impulsiv og antisosial adferd: antisosial personlighets-forstyrrelse

14
Composite index of antisocial behavior (z scores).
(From Caspi et al. Science 2002; 297; )
")
15
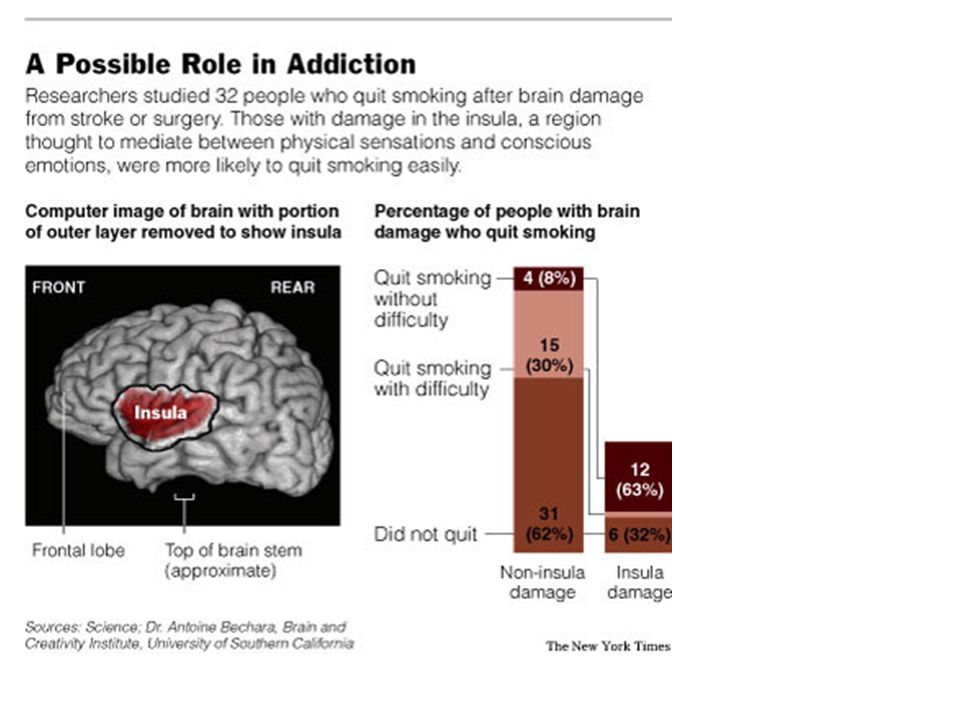
F45.0 Panic disorder 48% Social phobia 34% OCD 11% Depression 66%
Problem: psychobiological studies of Briquets syndrome / somatization” are seldom ”clean” Example comorbidity in one study: F45.0 Panic disorder % Social phobia % OCD % Depression % Bulimia % Rief et al, Psychosom Med 1998; 60:

16
Somatoform disorders Stressfysiologi- personlighet

17
Stress Sentralnervesystemet Kognitive-emosjonelle forhold
Fysiologisk Adferd aktivering Kommunikasjon Klassisk betinging Operant betinging Miljø Arv Funsjonelle somatiske lidelser

18
Genetic variance in the promoter region of the serotonin
transporter protein gene (SLC6A4): The genotype frequencies are 36% L/L, 48% L/S, and 16% S/S. Right amygdala activation is relatively greater in normals who have the S allele. S/S allele is associated with increased risk for depression and negative stress responses. Hariri AR, Brown SM. Am J Psychiatry 163:12, January 2006
: The genotype frequencies are. 36% L/L, 48% L/S, and 16% S/S. Right amygdala activation is. relatively greater in normals who have the S allele. S/S allele is. associated with increased risk for depression and negative stress responses. Hariri AR, Brown SM. Am J Psychiatry 163:12, January")
19
The association between childhood maltreatment (between
the ages of 3 and 11 years) and adult depression (ages 18 to 26), as a function of 5-HT Transporter genotype. Interaction analysis showed that childhood stress predicted adult depression only among individuals carrying an s allele Caspi et al. Science 18 July 2003: Vol no. 5631, pp
 and adult depression. (ages 18 to 26), as a function of 5-HT Transporter genotype. Interaction analysis showed that childhood stress predicted. adult depression only among individuals carrying an s allele. Caspi et al. Science 18 July 2003: Vol no. 5631, pp")
20
Social and reward frustration in real life:
Social and reward frustration in real life: The model of effort-reward imbalance at work (Siegrist 1996) wage, salary esteem promotion/ security demands / obligations reward effort motivation (‘overcommitment‘) motivation (‘overcommitment‘) Imbalance maintained → if no alternative choice available → if accepted for strategic reasons → if motivational pattern present (overcommitment)
 wage, salary. esteem. promotion/ security. demands / obligations. reward. effort. motivation. (‘overcommitment‘) motivation. (‘overcommitment‘) Imbalance maintained. → if no alternative choice available. → if accepted for strategic reasons. → if motivational pattern present (overcommitment)")
21
Mean systolic blood pressure (mmHg) in men over a working day according to overcommitment and occupational position (N=105) Source: A. Steptoe et al. (2004), Psychosomatic Medicine, 66:
, Psychosomatic Medicine, 66:")
22
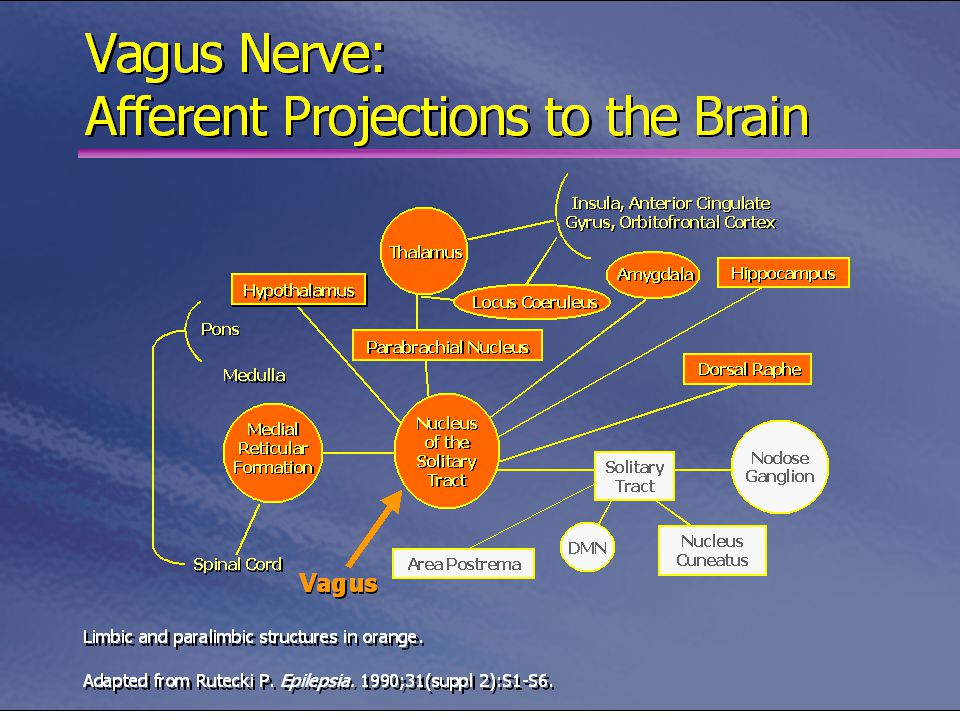
The neurophysiology of emotions
Neocortex, asossiation cortex Thalamus Cingular anterior cortex Hippocampus Amygdala BNST Autonomic centers (LC, vagus nuclei) ANS Hypothalamus, PVN HPA-axis Periaqueductal grey Behaviour
 ANS. Hypothalamus, PVN. HPA-axis. Periaqueductal grey. Behaviour.")
23
How does the brain deal with social reward? Brain reward system
prefrontal cortex orbitofrontal cortex anterior cingulate thalamus mesocortico-limbic dopamine system ( nucleus accumbens, hippocampus, amygdala, hypothalamus) Source: E.T. Rolls (2000), W. Schultz et al. (1997), R.A. Wise (2002).
 Source: E.T. Rolls (2000), W. Schultz et al. (1997), R.A. Wise (2002).")
24
but Effort-reward imbalance high risk vs. low risk group;
An fMRI-study (Siegrist J, et al. Neuroreport 2005; 16: ) ERI high risk vs low risk: No diff in mental arithmetic performance, intelligence, or mood but diff between ERI high risk and low risk in following regions of the brain reward system: increased activity: thalamus (T = 4.6; p = .003); anterior cingulate (T = 3.7; p = .026); dorsolateral prefrontal cortex (T = 3.5; p = .034) reduced activity: hippocampus (T = 3.7; p = .026)
 ERI high risk vs low risk: No diff in mental arithmetic performance, intelligence, or mood. but. diff between ERI high risk and low risk in following regions. of the brain reward system: increased activity: thalamus (T = 4.6; p = .003); anterior cingulate (T = 3.7; p = .026); dorsolateral prefrontal cortex (T = 3.5; p = .034) reduced activity: hippocampus (T = 3.7; p = .026)")
25
fMRI results Siegrist J, et al. Neuroreport 2005; 16: 1899-1903
Increased activity in anterior cingulate (bilateral) in the Effort-reward imbalance high risk vs. low risk group; z = 16; p = .001 (uncorrected); p < .05 (small volume corrected)
 in the Effort-reward imbalance high risk vs. low risk group; z = 16; p = .001 (uncorrected); p < .05 (small volume corrected)")
26
De Gucht et al J Psychosom Res 2004; 279: 279-285
Personlighet og mangeårige medisinsk ”uforklarlige” kroppslige symptomer 6 mndrs. oppfølging av almenpraksispas. ;( n=318) Prediksjon av økning i symptomer OR Nevrotisisme (NEO-PI; nevrotisisme subskala) Alexithymi (TAS-20) Økende negativ affekt (Positive and Negative Affect Schedule) Økende positiv affekt Prediksjon av vedvarende høyt antall symptomer Kvinne Nevrotisisme Vanskelig å beskrive følelser 1.08 Høy negativ affekt Høy positiv affekt De Gucht et al J Psychosom Res 2004; 279:
 Prediksjon av økning i symptomer. OR. Nevrotisisme 1.03 (NEO-PI; nevrotisisme subskala) Alexithymi 1.00 (TAS-20) Økende negativ affekt 1.78 (Positive and Negative Affect Schedule) Økende positiv affekt Prediksjon av vedvarende høyt antall symptomer. Kvinne Nevrotisisme Vanskelig å beskrive følelser Høy negativ affekt Høy positiv affekt De Gucht et al J Psychosom Res 2004; 279:")
27
Cardiovascular response and hostility
Change in BP during recovery [mm Hg] Change in HR during task [BPM] Suarez et al, Psychosom Med 1998; 60: 78-88

28
The “high” Neuroticism personality
anxious worrying moody sleep badly overly emotional sensitive to environmental stimuli reactions are often irrational and occasionally rigid Psychosomatic symptoms are common

29
hCRH-stimulation test in pts with high and low neuroticism
DCOR nmol/l McCleery & Goodwin Biol Psych 2001; 49: 410-5 Mean score: [SD 2.2] [SD 2.0]

30
Fysiologisk fellesnevner::::::::::::::::::::::::::::::::::::::::::::::::?????

33
The brain-gut network Frontal brain hypersensitivity Emotions Stress
Vulnerability Spinal afferents Gut hypersensitivity - receptorer i mucosa -receptorer i tarmvegg Infection IBD

34
Frontal brain reactivity to anxiety words in pts with IBS
N400 to anxiety and sadness words deeper in IBS patients than controls (p<.0.01). N400 to anger words threshold significant (p=0.053) Rectal wall reactivities to anger and anxiety words predicted N400 amplitudes in total sample (p<0.01) Significant predictions (gut/brain) appeared only between reactivities to the same word series. Blomhoff et al Scand J Gastroent 2000; 35: Digest Dis Scienc ; 45:1153-9 Digest Dis Science 2000; 45:
. N400 to anger words threshold significant (p=0.053) Rectal wall reactivities to anger and anxiety words predicted N400 amplitudes in total sample (p<0.01) Significant predictions (gut/brain) appeared only between reactivities to the same word series. Blomhoff et al. Scand J Gastroent 2000; 35: Digest Dis Scienc 2000; 45: Digest Dis Science 2000; 45:")
35
Depressive and anxiety symptoms in patients with IBS, NUD and FM compared with health controls. A metaanalysis of / studies. (Henningsen et al, Psychosom Med 2003; 65: ).
..")
36
Mental disorders among women with ”psychosomatic syndromes”
Eva Malt et al. J Psychosom Res 2000;

37
Fibromyalgia vs healthy
controls Wood. Int Review Neurobiology 2005; 67:

38
of innocuous pressure. Overlapping activations: yellow
S=Somatosensorisk cortex (I: primary; II: secondary) Inferior parietal lobe superior temporal gyrus Common regions of activation (fMRI) in patients (red) and in the subjective pain control condition (green), in which the effects of pressure applied to the left thumb sufficient to evoke a modrate pain rating are compared with the effects of innocuous pressure. Overlapping activations: yellow Arrows: rCBF increase (decrease) Wood. Int Review Neurobiology 2005; 67:
 Inferior parietal lobe superior temporal gyrus. Common regions of activation (fMRI) in patients (red) and in the subjective pain. control condition (green), in which the effects of pressure applied to the left. thumb sufficient to evoke a modrate pain rating are compared with the effects. of innocuous pressure. Overlapping activations: yellow. Arrows: rCBF increase (decrease) Wood. Int Review Neurobiology 2005; 67:")
39
Nevrobiologi og alexithymi
Genetisk? Hemisfærekommunikasjon? Traumenevrobiologi?

40
Somatoform disorders Klassisk betinging

41
Anfallvise psykiske lidelser
Stress Sentralnervesystemet Kognitive-emosjonelle forhold Fysiologisk Adferd aktivering Kommunikasjon Klassisk betinging Operant betinging Miljø Arv Funsjonelle somatiske lidelser

42
Pavlovian conditioning (”unconscious memory”)
Important issues Brain structures e.g. amygdala-olfactorial and contextual fear conditions; perirhinal cortex-olfactorial conditioning Dopamin, NMDA-receptors Type of conditioned stimulus e.g. olfactory, facial expression Otto et al, Behav Brain Res 2000; 110:

43
Glucosechange in response to saline after 4 days of olfactory conditioning with insulin
Blood glucose mg/dl 20 healthy subjects 20-30 years of age Stockhorst et al, Psychosom Med 1999; 61:424-35

44
Brain Response to Visceral Aversive Conditioning A) Generic brain
Yágüez et al. Gastro- Enterology 2005; 128: A) Generic brain activation during the learning phase, ie, painful esophageal distention B) Anticipation phase C) Extinction phase Note the activation of the insula, right inferior frontal gyrus, and anterior cingulate cortex (ACC) in (A), (B), and (C). Activation in the dorsolateral prefrontal cortex (DLPFC) was found only in the (B) anticipation and (C) extinction phase.
 Generic brain. activation during. the learning phase, ie, painful esophageal. distention. B) Anticipation phase. C) Extinction phase. Note the activation of the. insula, right inferior frontal. gyrus, and anterior cingulate. cortex (ACC) in (A), (B), and. (C). Activation in the. dorsolateral prefrontal cortex. (DLPFC) was found only in. the (B) anticipation and (C) extinction phase.")
45
Somatoforme tilstander: Nevrobiologi
Psykiske sykdommer: nevrobiologi som også impliserer somatiske symptomer / syndromer

47
Affektivt fMRI paradigme: emosjonelt negative og nøytrale bilder
Koronalt snitt som viser bilateral amygdala-aktivering ved emosjonelt negative stimuli (differanse i aktivering negative – nøytrale bilder). Grønn = friske kontroller (n=4), rød = RBD-pas. (n=6) Egne data; preliminære
. Grønn = friske kontroller (n=4), rød = RBD-pas. (n=6) Egne data; preliminære.")
48
Legemlige symptomer ved depresjoner
Trett, utslitt Sensoriske symptomer eks. parestesier, svimmelhet, uklart syn etc Gastrointestinale symptomer eks. dyspepsi-plager, svelg-plager, forstoppelse Smerter Diffuse smerter, hodepine, migrene (Andre) autonome symptomer eks. cor
 autonome symptomer eks. cor.")
49
The percentage of individuals meeting diagnostic
criteria for depression at age 26, as a function of 5-HT Transporter genotype and number of stressful life events between the ages of 21 and 26. Short genotype: S/S; S/L Long genotype: L/L Caspi et al. Science 18 July 2003: Vol no. 5631, pp

50
Areas in the cingulate (right) and amygdala (left) that differed in gray
matter volume between subjects with the short and long version version of the serotonin transporter gene. Short version carriers showed the greatest reductions in the red area, which previous studies have linked to depression. (Image courtesy of National Institute of Mental Health) serotonin/gene-brain.html
 serotonin/gene-brain.html.")
51
Egne undersøkelser: PNES vs ”psykosomatiske” og friske pasienter
PNES flere psykiske lidelser pr. pasient (1.9 vs 1.5; p=0.003) PNES = Somatoforme lidelser mtp angst / depresjon > friske 10/23 av PNES pasientene hadde somatoform smertelidelse Mer aggresjon /fiendtlighet hos PNES (forbundet med øket forekomst av personlighetsforstyrrelser) Møkleby et al. Epilepsia 2002; 43: 193-8
 PNES = Somatoforme lidelser mtp angst / depresjon > friske. 10/23 av PNES pasientene hadde somatoform smertelidelse. Mer aggresjon /fiendtlighet hos PNES (forbundet med øket forekomst av personlighetsforstyrrelser) Møkleby et al. Epilepsia 2002; 43:")
52
Respiratory dysfunction in PD, GAD and controls
Tidal Volume mL Inspiratory Flow rate mL/sec Sighs >2 (number/ Min x 100) All differences are stat.significant Wilhelm et al, Biol Psychiatry 2001; 49:
 All differences are stat.significant. Wilhelm et al, Biol Psychiatry 2001; 49:")
53
Neurologic Soft Signs in Chronic PTSD (Tamara et al
Neurologic Soft Signs in Chronic PTSD (Tamara et al. Arch Gen Psychiatry. 2000;57: )
")
54
(Unstable personality Disorder)
Borderline Personality Disorder (Unstable personality Disorder) Psykosomatiske symptomer Maclashan et al, 2005
 Psykosomatiske. symptomer. Maclashan et al,")
55
Examples PNES more personality disorders than clinical and non-clinical controls. Borderline personality disorder> overly controlled personality >avoidant personality disorder (few). (Reuber et al. J Neurol Neurosurg Psychiatry. 2004;75:743-8)
. (Reuber et al. J Neurol Neurosurg Psychiatry. 2004;75:743-8)")
56
Borderline Personality Disorder (DSM-IV)
Figure 4. Scatter plot of left and right hippocampal volumes (mL) for subjects with borderline personality disorder and healthy control subjects. Group means are indicated by horizontal lines (Irle et al. Biolog Psych 2005; 57: )
 for subjects. with borderline personality disorder and healthy control subjects. Group means. are indicated by horizontal lines (Irle et al. Biolog Psych 2005; 57: )")
57
Significant volume reduction in (A) left orbitofrontal and (B) right anterior
cingulate gyrus in patients with borderline personality disorder (BPD) and healthy controls (HC) (horizontal BAR = mean; BOX = 95% confidence interval). (van Elst et al, Biological Psychiatry 2003; 54: ).
 and. healthy controls (HC) (horizontal BAR = mean; BOX = 95% confidence. interval). (van Elst et al, Biological Psychiatry 2003; 54: ).")
58
Activation map showing regions in the amygdala slice in which
activation exceeded the criterion threshold level of p < .005 for the normal control and borderline personality disorder groups for each of the four facial expressions (Donegan et al, Biol Psychiatry 2003; 54: )
")
59
Repeated measures analysis of variance revealed increased cortisol, tumor necrosis
factor-α (TNF-α), and interleukin-6 (IL-6) in serum profiles of patients with comorbid current major depressive disorder and borderline-personality disorder (MDD/BPD). *Indicates significant differences between the groups obtained by pairwise post-hoc analysis (p < .05). CG, comparison group. (Kahl et al, Biolog Psychiatry 2005)
, and interleukin-6 (IL-6) in serum profiles of patients with comorbid. current major depressive disorder and borderline-personality disorder (MDD/BPD). *Indicates significant differences between the groups obtained by pairwise post-hoc. analysis (p < .05). CG, comparison group. (Kahl et al, Biolog Psychiatry 2005)")
Liknende presentasjoner