Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Utvikling over livsløpet
Inger Hilde Nordhus

2
Livsløp og utvikling (1)
Aldring er generelt beskrevet som en prosess preget av svekkelse Psykologisk forskning støtter i stor grad dette: Arbeidsminne – (multiple oppgaver) og informasjonsbearbeiding (hurtighet) svekkes Erfaringsbasert kunnskap viser ikke denne tendensen men det gjør derimot prosessering av ny kunnskap Etablert på tvers av kjønn, utdanning og etnisk tilhørighet – normative endringer med store individuelle forskjeller National Research Council The Aging Mind: Directions in Cognitive Aging Research . P. Stern & L. L. Carstensen, Eds. National Academies of Sciences Press. Washington, DC.
 og informasjonsbearbeiding (hurtighet) svekkes. Erfaringsbasert kunnskap viser ikke denne tendensen men det gjør derimot prosessering av ny kunnskap. Etablert på tvers av kjønn, utdanning og etnisk tilhørighet – normative endringer med store individuelle forskjeller. National Research Council The Aging Mind: Directions in Cognitive Aging Research . P. Stern & L. L. Carstensen, Eds. National Academies of Sciences Press. Washington, DC.")
3
Patologisk kognitiv utvikling - demens
Svært varierende prevalens av demens rundt om i verden (3-30 % av eldre) 1-5 Klassifikasjonssystemene påvirker diagnosen6 I en canadisk kohort varierte prevalensen fra 3,1 % (ICD-10) til 29,1 % (DSM-III)6 Prevalens i vestlige land:7-8 Norske sykehjem:9 70-74 år = 5 % > 75 år = 15 % > 90 år = 35 % Shaji S et al. An epidemiological study of dementia in a rural community in Kerala, India. Br J Psychiatry. 1996;168(6):745-9. Wang W et al. Prevalence of Alzheimer's disease and other dementing disorders in an urban community of Beijing, China. Neuroepidemiology Jul-Aug;19(4): Lobo A et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S4-9. Engedal K and Haugen PK. The prevalence of dementia in a sample of elderly Norwegians. International Journal of Geriatric Psychiatry 1993;8: Skoog I et al. A population-based study of dementia in 85-year-olds. N Engl J Med. 1993;21: 70-80 % Engedal K, Haugen PK. The prevalence of dementia in a sample elderly Norwegians. Int J Geriatr Psychiatry 1993;8: Ott A et al. Prevalence of Alzheimer's disease and vascular dementia: association with education. The Rotterdam study. BMJ. 1995;15: 9. Nygaard H et al. Mental svikt hos sykehjemspasienter. Tidsskr Nor Lægeforen 2000;120: Erkinjuntti T et al. The effect of different diagnostic criteria on the prevalence of dementia. N Engl J Med. 1997;4:
 1-5. Klassifikasjonssystemene påvirker diagnosen6. I en canadisk kohort varierte prevalensen fra 3,1 % (ICD-10) til 29,1 % (DSM-III)6. Prevalens i vestlige land:7-8. Norske sykehjem: år = 5 % > 75 år = 15 % > 90 år = 35 % Shaji S et al. An epidemiological study of dementia in a rural community in Kerala, India. Br J Psychiatry. 1996;168(6): Wang W et al. Prevalence of Alzheimer s disease and other dementing disorders in an urban community of Beijing, China. Neuroepidemiology Jul-Aug;19(4): Lobo A et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S4-9. Engedal K and Haugen PK. The prevalence of dementia in a sample of elderly Norwegians. International Journal of Geriatric Psychiatry 1993;8: Skoog I et al. A population-based study of dementia in 85-year-olds. N Engl J Med. 1993;21: % Engedal K, Haugen PK. The prevalence of dementia in a sample elderly Norwegians. Int J Geriatr Psychiatry 1993;8: Ott A et al. Prevalence of Alzheimer s disease and vascular dementia: association with education. The Rotterdam study. BMJ. 1995;15: Nygaard H et al. Mental svikt hos sykehjemspasienter. Tidsskr Nor Lægeforen 2000;120: Erkinjuntti T et al. The effect of different diagnostic criteria on the prevalence of dementia. N Engl J Med. 1997;4:")
4
Livsløp og utvikling (2)
Sosial og emosjonell fungering viser positiv utvikling over livsløpet (med unntak av ved patologisk aldring) Subjektivt velvære (well-being) er ikke dårligere hos eldre enn yngre voksne Negative emosjoner viser nedgang relativt til yngre voksne; positive emosjoner rapporteres oftere hos eldre enn yngre voksne Eldre rapporterer oftere større grad av tilfredshet mht sosiale relasjoner, særlig nære (slekt og nære venner) Sett opp mot kognisjon og biologiske prosesser: paradox of aging ? Löckenhoff, C. E. & L. L. Carstensen Is the life-span theory of control a theory of development or a theory of coping? I Personal Control in Social and Life Contexts. S. H. Zarit, L. I. Pearlin & Schaie, Eds.: Springer Publishing Company. New York.
 Subjektivt velvære (well-being) er ikke dårligere hos eldre enn yngre voksne. Negative emosjoner viser nedgang relativt til yngre voksne; positive emosjoner rapporteres oftere hos eldre enn yngre voksne. Eldre rapporterer oftere større grad av tilfredshet mht sosiale relasjoner, særlig nære (slekt og nære venner) Sett opp mot kognisjon og biologiske prosesser: paradox of aging Löckenhoff, C. E. & L. L. Carstensen Is the life-span theory of control a theory of development or a theory of coping I Personal Control in Social and Life Contexts. S. H. Zarit, L. I. Pearlin & Schaie, Eds.: Springer Publishing Company. New York.")
5
Psykologiske mekanismer
Senket forventning Endring av referansegruppe Benekting Med andre ord: ……en grunnleggende oppfatning av: at økt emosjonell trivsel og fokus på nære bånd hos eldre er et utslag av mestring av tap mer enn en positiv utvikling

6
Selektiv motivasjon – et utviklingsperspektiv
Mål rettet mot å utvide vår horisont/få mer informasjon Mål rettet mot emosjonell bekreftelse Evne til å oppleve seg i tid gjør at en også kan endre prioritet Med andre ord: ……en alternativ oppfatning av: at økt emosjonell trivsel og fokus på nære bånd hos eldre er et utslag av relativ endring i prioritering av mål

7
Selvregulering over livsløpet
Selvregulering hos barn blir beskrevet i et utviklingsperspektiv Selvregulering hos voksne og eldre tar lite hensyn til ontogenetisk endring over livsløpet Fokus på voksne: individuelle forskjeller Fokus på eldre: Sviktende fysisk helse forårsaker dysfunkjonell selvregulering

8
Oppsummerende I klinisk sammenheng vil vi selvsagt se store individuelle endringer i evne til selvregulering hos voksne og eldre pasienter Vi vil også bli konfrontert med klare sammenhenger mellom fysisk helsesvikt og psykisk helse De generelle funn om eldres selvregulering peker imidlertid mer mot psykologisk gevinst enn mot en normativ defensiv mestring av tap

9
Ageing – Health – Behaviour
Optimize life expectancy or longevity Minimize physical, psychological and social morbidity Increase of people surviving into advanced old age leads to compression of morbidity (disease closer to the time of death) Can we live free from disease?
 Can we live free from disease")
10
Health and Disease Age is linked to many diseases (e.g., heart disease, dementia) Diseases have a number of psychological consequences The fact that people live longer also implies an increase in both healthy as well as abnormal ageing Health is also known to be the main determinant of life satisfaction and quality of life in old age

11
Is Old Age Synonymous with Disease?
How do we perceive ageing? What kind of images of old age do we have? What do we think of as normal ageing?

12
Age Immediate information about somebody we do not know
Strong association with other variables Subjective marker (e.g., change) Social marker (e.g., being different from younger adults)
 Social marker (e.g., being different from younger adults)")
13
Age as a variable Age as a statistical concept Age as a process
Age as a background variable Age as a predictor variable

14
What is Ageing? Biological perspective (cell loss, physiological changes) Developmental perspective (coping, adaptation) Cognitive perspective (memory, attention) Social perspective (status, resources)
 Social perspective (status, resources)")
15
Biological Age Observable physical changes Changes in the brain
Increased vulnerability for developing certain ailments and diseases

16
Sleep – an example Certain changes in the sleep architecture are defined as common and normal as we age Changes in sleep habits Changes in activity level Prevalence of sleep problems increases with age, and about 50% of elderly subjects (60+) complain about sleep problems Why? Aktivitetsnivå og forskning: Generelt viser ikke forskning noen klarer sammenhenger mellom fysisk aktivitet og søvn
 complain about sleep problems. Why Aktivitetsnivå og forskning: Generelt viser ikke forskning noen klarer sammenhenger mellom fysisk aktivitet og søvn.")
17
Sleep in old age Sleep changes naturally as we age
Increased number of awakenings and arousals Less REM sleep Generally less deep sleep Moe sleep stage changes Less sleep cycles Reduced sleep efficacy

18
Sleep - Normal Changes in Sleep Architecture

19
Actigraphy

20
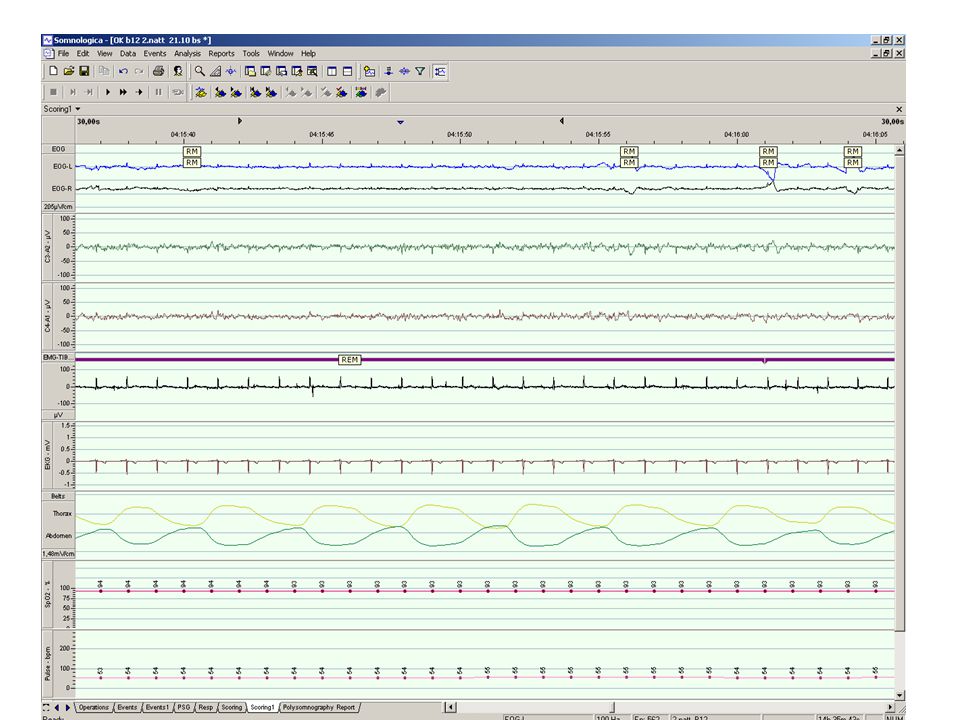
Polysomnography (1) Polysomnography
 Polysomnography")
21
Polysomnography (2)
")
23
Sleep Diary Uke: fra .......... til ........... År:...........
Eksempel Mandag Tirsdag Onsdag Torsdag Fredag Lørdag Søndag Utfyllingsdato (fylt ut om morgenen den) / / / / / / /3 1. Antall ganger jeg sov (duppet av) på dagtid (før natten) 2. Hvor lenge jeg sov (duppet av) på dagtid 3. Om kvelden la jeg meg i sengen kl 4. Etter jeg la meg prøvde jeg å sove (slukket lysene) kl 5. Etter å ha slukket lyset, sovnet jeg i løpet av… minutter min 6. Antall ganger jeg våknet i løpet av natten var 7. Hvor lenge jeg var våken til sammen om natten (legg sammen for alle oppvåkninger) 8. Jeg våknet endelig kl (siste oppvåking om morgenen) 9. Jeg stod endelig opp av sengen kl 10. På dagtid i går følte jeg meg (1= svært søvnig, 2= noe søvnig, 3 = hverken søvnig eller opplagt, 4 = noe opplagt, 5= svært opplagt) 11. Da jeg stod opp i morges følte jeg meg (1= helt utslitt, 2= noe utslitt, 3= hverken utslitt eller uthvilt, 4= noe uthvilt, 5 = helt uthvilt) 12. Jeg inntok … enheter alkohol før jeg la meg (eks på enhet = én pils, et glass vin, én drink brennevin)
 27/2 28/2 1/3 2/3 3/3 4/3 5/3. 1. Antall ganger jeg sov (duppet av) på dagtid (før natten) Hvor lenge jeg sov (duppet av) på dagtid Om kvelden la jeg meg i sengen kl Etter jeg la meg prøvde jeg å sove (slukket lysene) kl Etter å ha slukket lyset, sovnet jeg i løpet av… minutter 30 min. 6. Antall ganger jeg våknet i løpet av natten var Hvor lenge jeg var våken til sammen om natten. (legg sammen for alle oppvåkninger) Jeg våknet endelig kl (siste oppvåking om morgenen) Jeg stod endelig opp av sengen kl På dagtid i går følte jeg meg (1= svært søvnig, 2= noe søvnig, 3 = hverken søvnig eller opplagt, 4 = noe opplagt, 5= svært opplagt) Da jeg stod opp i morges følte jeg meg (1= helt utslitt, 2= noe utslitt, 3= hverken utslitt eller uthvilt, 4= noe uthvilt, 5 = helt uthvilt) Jeg inntok … enheter alkohol før jeg la meg (eks på enhet = én pils, et glass vin, én drink brennevin) 2.")
24
Ageing as a health related concept
Pathological – normal- optimal Heterogeneity Risk Vulnerability

25
Psychological Age Changes in cognitive preparedness
Increased vulnerability in terms of critical incidences Increased vulnerability in terms of loss of resources that in turn challenge coping and adaptation

26
What may challenge identity and coping in old age?
Interpersonal loss Physical decline and loss and malfunction Increased dependency of care Fear of loosing autonomy and integrity Affects basic human needs

27
Social Age Changes in roles and status
Increased likelihood of being in a position of a recipient in many ways Exit from roles rather than entrance into roles as defined by

28
Age, Cognitive Functioning and Health
The most feared diseases of old age are those that impair memory, thinking, problem-solving, perception and our personality It is a challenge to understand the borderlands between benign cognitive impairment and abnormal cognitive functioning (dementia )
")
29
A Healthy Old Age? There is little evidence for marked compression of morbidity The absolute time spent with moderate disability has increased More people are able to perform activities of daily living due to medical and technological improvement As for cognition, at least some decline is the norm, but there are great inter-individual variation

30
Age as a Mediator between Health and Behaviour
It is well established that before old age, behaviour has both beneficial and negative effects on health Smoking, alcohol abuse, poor diet, obesity, lack of exercise, etc., reduce the likelihood of surviving into old age The debate in gerontology is whether risk factors associated with mortality and morbidity in middle age has as strong effect in old age

31
Two Conclusions: There is evidence that behaviour change in old age has a beneficial effect on health and psychological well-being It may also be the case that the same levels of behaviour in old age are more harmful than at younger ages

32
The Issue of Self-Efficacy
There is a growing body of evidence demonstrating the role of age as a mediator between behaviour and health: One possible mechanism might be changes in perceived self-efficacy or control over health with age There is some evidence that here are decreases in perceived self-efficacy with age: Ageing or cohort?

33
”Elderly ” Persons 60+ (arbitrary limit) Chronological definition
Social definition The experience of being old Related to indentity

34
A correction The health status of those 60+ is better than ever
Most elderly people can mange without any particular help Ageing is not identical with disease Aged people are not a homogenous group

35
Optimal ageing Optimal Ageing: ”The potential and preparedness for dealing with change” (Kilde: Baltes & Baltes, 1993). Discuss this statement

36
Ageing may imply Narrowing of choices as a consequence of loss
Coping relates to use strategies that has proven to be effective earlier in life Coping may also mean to develop or reformulate old strategies to make them fit in a new context

37
Critical Life Events Resources Stressors Social Social Psycological
Biological Social Psycological Biological Resources Stressors

Liknende presentasjoner





>")













