Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Antibiotics In Modic changes; The AIM-study
Antibiotic treatment in patients with chronic low back pain and Modic Changes a randomized controlled trial Antibiotics In Modic changes; The AIM-study Kjersti Storheim, OUS Ullevål And the Norwegian AIM study group

2
Background Low back pain (LBP) is the number one cause for living with disability globally Huge expenses Most patients are viewed within a biopsychosocial model and are not given a patho-anatomical diagnosis Treatment effects for non-specific LBP are in general small – moderate

3
Background Albert et al treated a sub-group of chronic LBP patients with a supposed biomedical source of LBP (Modic Changes) with Amoxicillin for 100 days The effect was substantially greater than all currently established treatments for chronic LBP RMDQ during study (range 0-23): baseline, 100 days, 1 year antibiotic 15, 11, 5.7 placebo 15, 14, 14 Leg pain during study (range 0 -10): baseline, 100 days, 1 y antibiotics 5.3, 3.0, 1.4 placebo 4.0, 4.3, 4.3 Lumbar pain during s (range 0 – 10): baseline, 100 days, 1 y antibiotics 6.7, 5.0, 3.7 placebo 6.3, 6.3, 6.3
 with Amoxicillin for 100 days. The effect was substantially greater than all currently established treatments for chronic LBP. RMDQ during study (range 0-23): baseline, 100 days, 1 year. antibiotic 15, 11, 5.7. placebo 15, 14, 14. Leg pain during study (range 0 -10): baseline, 100 days, 1 y. antibiotics 5.3, 3.0, 1.4. placebo 4.0, 4.3, 4.3. Lumbar pain during s (range 0 – 10): baseline, 100 days, 1 y. antibiotics 6.7, 5.0, 3.7. placebo 6.3, 6.3, 6.3.")
4
Background The Danish study may be a potentially important breakthrough in the understanding and management of LBP Evoked parallels to the discoveries that a chronic Helicobacter pylori infection of the stomach lining causes % of ulcers

5
Modic Changes (MCs) The hypothesis of the Danish study
Type 1: Ødem Type 2: Fettomdanning Type 3: Sclerose Modic Changes (MCs) Visible on MRI-scans only Classified into type I, II and III Frequent finding in patients with LBP Sign risk factor for LBP (Jensen et al 2012, Määttä et al 2015) The aetiology and pathogenesis is unclear Mechanical? (the forces acting within the disc)inflammatory reaction Nucleus tissue entering the vertebrae cause an autoimmune reaction? MCs occur due to edema surrounding an infected disc? infection with low virulent anaerobic organisms, mainly the propionibacterium acnes (P.acnes) is found in biopsies from nucleus material i.e. the infection is in the disc and the MC is a secondary change in the bone due to cytokine and propionic acid production The hypothesis of the Danish study MCs can be treated by antibiotic
 Visible on MRI-scans only. Classified into type I, II and III. Frequent finding in patients with LBP. Sign risk factor for LBP (Jensen et al 2012, Määttä et al 2015) The aetiology and pathogenesis is unclear. Mechanical (the forces acting within the disc)inflammatory reaction. Nucleus tissue entering the vertebrae cause an autoimmune reaction MCs occur due to edema surrounding an infected disc infection with low virulent anaerobic organisms, mainly the propionibacterium acnes (P.acnes) is found in biopsies from nucleus material. i.e. the infection is in the disc and the MC is a secondary change in the bone due to cytokine and propionic acid production. The hypothesis of the Danish study. MCs can be treated by antibiotic.")
6
Criticism….. The prevalence of MCs is high
40-50% in LBP patients 10-20% in normal populations: Kjær 2005, Jensen 2009, Jensen 2009, Mättää et al 2015 Use of antibiotics in a large patient group… Can cause risky antibiotic side effects in individuals May spread antibiotic resistance Jensen et al 2008

7
Criticism…. The MRI-based selection of patients for antibiotic treatment is not without problems The type of MCs (especially type I vs. II) has been used to guide on treatment Albert et al included only patients with type I MCs low field 0.2 T The differentiation between type I and II may be less relevant, since the different types of MCs may represent different stages of a common process Also, there are important challenges when evaluating Modic type Different observers may report up to twofold different prevalence of MCs (any type) at a specific endplate (e.g. 25% vs. 50%)
 has been used to guide on treatment. Albert et al included only patients with type I MCs. low field 0.2 T. The differentiation between type I and II may be less relevant, since the different types of MCs may represent different stages of a common process. Also, there are important challenges when evaluating Modic type. Different observers may report up to twofold different prevalence of MCs (any type) at a specific endplate (e.g. 25% vs. 50%)")
8
Betydning av magnetfeltstyrke
Signalet fra fett og vann avhenger av feltstyrken Høyt magnetfelt gir kraftigere signal, men også mer artefakter. T1 og T2 egenskapene er også feltavhengige Modic type 1 var 3 x hyppigere ved lav feltstyrke Modic type 3 var 2 x hyppigere ved høy feltstyrke Bendix et al 2012

9
Criticism….. It is not clear how nucleus pulposus and/or “infection fluids” leak into the endplates and become manifested as MCs in the bone Biological material analysed for bacteria is harvested from patients having surgery we cannot rule out that the bacteria found in the nuclear material may be due to intraoperative contamination rather than infection

12
No change in the Placebo group
RMDQ : antibiotic 15, 11, 5.7 placebo 15, 14, 14 Leg pain : antibiotics 5.3, 3.0, 1.4 placebo 4.0, 4.3, 4.3 Lumbar pain : antibiotics 6.7, 5.0, 3.7 placebo 6.3, 6.3, 6.3

13
Hence…. A new RCT should be performed to prevent inappropriate use of antibiotics in a large group of patients based on a single trial.

14
Aims The overall aim of the present study is to re-examine the finding that antibiotic treatment can cure patients with chronic LBP and MCs Further, to add important new knowledge to the research field beyond the Danish RCT broadening the inclusion criteria to include both patients with type I and type II MCs by improving the MRI assessment of MCs contribute to a clarification of the pathogenesis of MCs by studying gene expression of inflammatory biomarkers to conduct health economic analysis to study effect-modifying factors

15
Methods Placebo-controlled RCT Multicenter UNN St.Olavs Hospital
Haukeland University Hospital Oslo University Hospital Drammen Hospital Østfold Hospital

16
Prosjektets organisering
Benedicte A Lid Ansgar Espeland PI’s UNN Audny Anke St.Olav Øystein Nygaard HUS Jan Sture Skouen Drammen Anne Froholdt Østfold Lars Grøvle OUS Jens Ivar Brox

17
Elektronisk datainnsamling

18
Participating hospitals
OUS Ullevål Coordinating investigator: John-Anker Zwart Project managing: Kjersti Storheim Local (and national) coordinating: Monica Wigemyr (Linda M Pedersen: blood /epigenetics) Principal Investigator (PI): Jens Ivar Brox (Elina Schistad / Lars CH Bråten / Mads Rolfsen / Bendik Winsvold) Haukeland US MR-imaging (Ansgar Espeland / Nils Vetti / Per M Kristoffersen) Infection medicine (Olav Lutro) / statistician (Jörg Aßmus) PI: Jan Sture Skouen (Thomas Kadar / Pål Christian Haugland / Tonje Wåle Flørenes / Siv K Claussen)
 coordinating: Monica Wigemyr (Linda M Pedersen: blood /epigenetics) Principal Investigator (PI): Jens Ivar Brox (Elina Schistad / Lars CH Bråten / Mads Rolfsen / Bendik Winsvold) Haukeland US. MR-imaging (Ansgar Espeland / Nils Vetti / Per M Kristoffersen) Infection medicine (Olav Lutro) / statistician (Jörg Aßmus) PI: Jan Sture Skouen (Thomas Kadar / Pål Christian Haugland / Tonje Wåle Flørenes / Siv K Claussen)")
19
Participating hospitals (cont)
Drammen hospital PI: Anne Froholdt (Sigrun Randen / Hilde Presberg) St.Olavs Hospital PI: Øystein Nygaard (Gunn Hege Marchand / Vidar Rao / Britt-Elin Lurud / Fredrik Granviken / Hege Andresen) Sykehuset Østfold PI: Lars Grøvle (Anne J Haugen / Knut Morten Huneide / Marianne Thorsø / Veronica Sørensen) Universitetssykehuset Nord-Norge (UNN) PI: Audny Anke (Terese Fors / Daniel Svendsen / Ingrid Knutsen
 St.Olavs Hospital. PI: Øystein Nygaard (Gunn Hege Marchand / Vidar Rao / Britt-Elin Lurud / Fredrik Granviken / Hege Andresen) Sykehuset Østfold. PI: Lars Grøvle (Anne J Haugen / Knut Morten Huneide / Marianne Thorsø / Veronica Sørensen) Universitetssykehuset Nord-Norge (UNN) PI: Audny Anke (Terese Fors / Daniel Svendsen / Ingrid Knutsen.")
20
Stipendiater Kliniske problemstillinger Radiologiske problemstillinger
Lars Christian Haugli Bråten (OUS Ullevål) Kjersti Storheim (hovedveileder) Radiologiske problemstillinger Per Martin Kristoffersen (Haukeland) Ansgar Espeland (hovedveileder) Epigenetikk / biomolekylært Maria Dehli Vigeland (OUS Ullevål / UiO) Benedicte A Lie (hovedveileder) Biopsier / histologi Mads Peder Rolfsen (OUS Ullevål) Christian Hellum (hovedveileder)
21
Case-control studie: biopsier
Case-control design Prøver både av ”sykt” og friskt vev Skivevev Bein Radiologi, blodprøver og epigenetikk som i RCT-studien Svært viktig supplement til RCT’en Finner vi anaerobe bakterier i skivevev / benvev?

22
Sikkerhetskomité (DMC)
Lege: Morten Lindbæk leder Antibiotikasenteret for primærmedisin (ASP). ASP ble opprettet i 2006 etter initiativ fra Folkehelseinstituttets komité for forebygging og bekjempelse av antibiotikaresistens (Antibiotikakomitéen). professor ved institutt for allmennmedisin, HELSAM. Etiker: Lisbeth Thoresen Avdeling for medisinsk etikk, UiO Statistiker: Are Hugo Pripp Avdeling for biostatistikk, epidemiologi og helseøkonomi Oslo universitetssykehus
. ASP ble opprettet i 2006 etter initiativ fra Folkehelseinstituttets komité for forebygging og bekjempelse av antibiotikaresistens (Antibiotikakomitéen). professor ved institutt for allmennmedisin, HELSAM. Etiker: Lisbeth Thoresen. Avdeling for medisinsk etikk, UiO. Statistiker: Are Hugo Pripp. Avdeling for biostatistikk, epidemiologi og helseøkonomi. Oslo universitetssykehus.")
23
Tidligere discoperert: JA / NEI
Strata for Modic type I / II Tidligere discoperert: JA / NEI

24
Tilvirkes av Kragerø Tablettproduksjon
Study interventions Antibiotic treatment: Amoxicillin 750 mgx3 for 100 days Versus placebo x3 for 100 days Tilvirkes av Kragerø Tablettproduksjon

25
Target population Patients from all health regions
Former disc herniation, now MC Both conservatively and surgically treated patients will be included If operated on for disc herniation, at least 12 months should have elapsed since surgery Patients registered in the Norwegian Registry for Spine Surgery operated on for disc herniation and reporting severe LBP pain at 12 months follow-up in the registry, will also be invited.

26
Inclusion criteria Aged between 18 and 65 years
LBP of > 6 months duration in the area below the 12th rib and above the gluteal folds with a Numerical Rating Scale (NRS) pain intensity score of 5 mean of three NRS scales; current LBP, the worst LBP within the last 2 weeks, and usual/mean LBP within the last 2 weeks. MRI-confirmed lumbar disc herniation within the preceding 2 years MC type I and/or type II in the vertebral body marrow at the same level as the previously herniated disc. For patients with former surgery for disc herniation, the MC has to be located at an operated level Written informed consent
 pain intensity score of 5. mean of three NRS scales; current LBP, the worst LBP within the last 2 weeks, and usual/mean LBP within the last 2 weeks. MRI-confirmed lumbar disc herniation within the preceding 2 years. MC type I and/or type II in the vertebral body marrow at the same level as the previously herniated disc. For patients with former surgery for disc herniation, the MC has to be located at an operated level. Written informed consent.")
27
Exclusion criteria Allergy to penicillin or cefalosporins
Allergy/hypersensitivity to any of the excipients of the study drug Current pregnancy or lactation Elevated kidney (creatinine) or hepatic (ALAT/ASAT) values outside normal range Phenylketonuria (Følling disease) Mononucleosis or leukaemia Any specific diagnosis that may explain patient’s low back symptoms (e.g. tumor, fracture, spondyloarthritis, infection, spinal stenosis). Former low back surgery (L1 – S1) for other reasons than disc herniation (e.g fusion, decompression, disc prosthesis).
 or hepatic (ALAT/ASAT) values outside normal range. Phenylketonuria (Følling disease) Mononucleosis or leukaemia. Any specific diagnosis that may explain patient’s low back symptoms (e.g. tumor, fracture, spondyloarthritis, infection, spinal stenosis). Former low back surgery (L1 – S1) for other reasons than disc herniation (e.g fusion, decompression, disc prosthesis).")
28
Exclusion criteria (cont)
Former surgery for disc herniation, but < 12 months have elapsed since surgery. Former surgery for disc herniation, but MC located at non-operated level(s) only. Reservation against intake of gelatine (the capsules contains gelatine, which among other things is produced by ingredients from pigs) Regular use of glucocorticoids Regular use of opioids with the exception of codeine and tramadol Not understanding Norwegian language Unlikely to adhere to treatment and/ or complete follow-up (e.g ongoing serious psychiatric disease, drug abuse, plans to move) Antibiotic treatment within the preceding one month before treatment start Contraindications to MRI (e.g. cardiac pacemaker electrodes, metal implant in eye or brain, claustrophobia). Unwilling to participate
 only. Reservation against intake of gelatine (the capsules contains gelatine, which among other things is produced by ingredients from pigs) Regular use of glucocorticoids. Regular use of opioids with the exception of codeine and tramadol. Not understanding Norwegian language. Unlikely to adhere to treatment and/ or complete follow-up (e.g ongoing serious psychiatric disease, drug abuse, plans to move) Antibiotic treatment within the preceding one month before treatment start. Contraindications to MRI (e.g. cardiac pacemaker electrodes, metal implant in eye or brain, claustrophobia). Unwilling to participate.")
29
Outcome measures Baseline variabler:
Primary outcome Roland Morris Disability Questionnaire Secondary outcomes Lumbar pain and leg pain measured by NRSs Bothersomeness Health-related quality of life (EuroQoL-5D) Days with sick leave Patient’s satisfaction Radiological outcomes Gene expression Cost-effectiveness Data will be collected at baseline, during treatment, post-treatment, during follow-up and at 1-year follow-up Baseline variabler: Demografi, etnisitet, subjektive helseplager, distress, fear-avoidance, smertetegning, forventning til effekt Blindingsindex: 100 dager, 1 år Main endpoint
 Days with sick leave. Patient’s satisfaction. Radiological outcomes. Gene expression. Cost-effectiveness. Data will be collected at baseline, during treatment, post-treatment, during follow-up and at 1-year follow-up. Baseline variabler: Demografi, etnisitet, subjektive helseplager, distress, fear-avoidance, smertetegning, forventning til effekt. Blindingsindex: 100 dager, 1 år. Main endpoint.")
30
Compliance to the medicine protocol, side-effects, and co-interventions (other pharmaco-logical treatment and non-pharmacological treatment) will also be registered Safety: Haematological blood samples, as well as kidney and liver function, will be assessed monthly during the intervention period, together with a short clinical evaluation (for monitoring patients clinical status related to antibiotic intake, not outcome measures).
.")
31
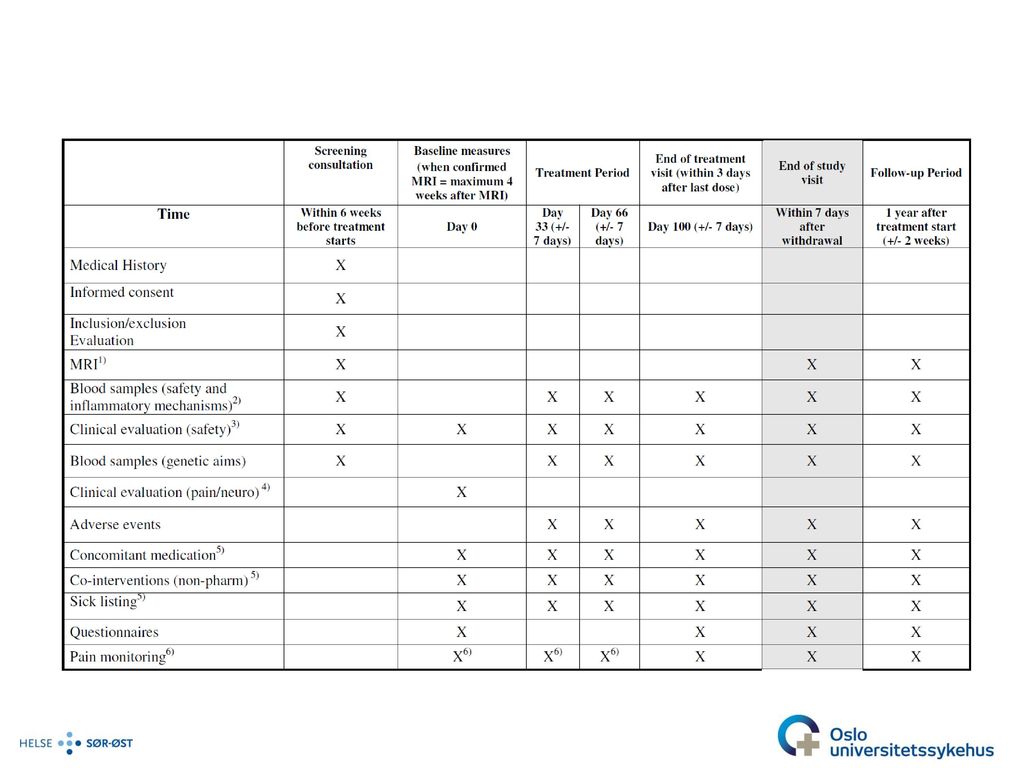
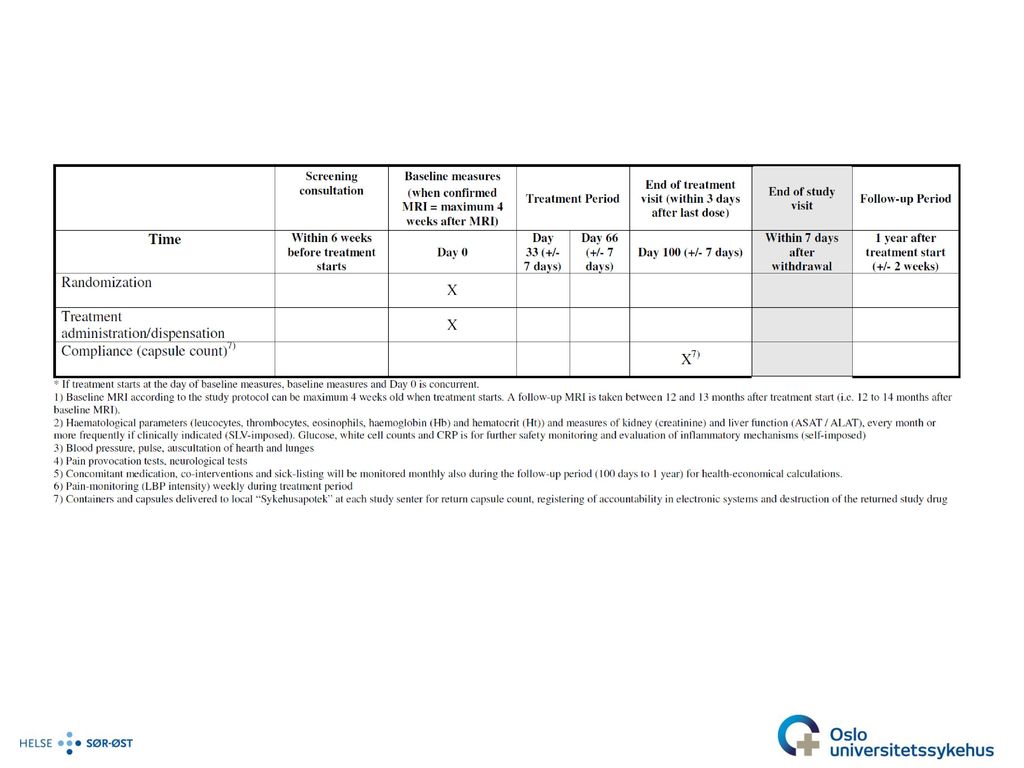
Tidslinje Behandling slutt = dag 100 Follow-up slutt Inklusjon = dag 0
1 år etter beh.start Inklusjon = dag 0 Klinisk ktr Dag 33 Klinisk ktr Dag 66 Screening Ny MR Behandlingsperiode Alle som tilfredsstiller alle inkl/ekskl krit og som henvises til nytt MR: MR-studier Ukentlig: Smertemonitorering og Compliance Månedlig helseøkonomi

32
Når kommer resultatene?
Ca 80 vurdert 33 startet behandlingen 14 inkluderbare Ca 10 henvist til MR etter studieprotokoll 2 års inklusjonsperiode? 1-års follow-up

33
Takk til Penger Egeninnsats

37
Trial Flow chart

Liknende presentasjoner
 til det europeiske kvalifikasjonsrammeverket EQF.>")





 happens in the database: : data.>")









 SGO1910 & SGO4930 Vår 2004 Foreleser: Karen O’Brien Seminarleder: Gunnar Berglund>")


