Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Spill for å trene – hva er kognitiv trening og har det effekt?
Phd Gro CC Løhaugen Spesialist i klinisk psykologi Nevropsykolog Leder HABU-Arendal HABU Arendal/Medisinsk fakultet NTNU

2
Hva er kognitiv trening?
1. Repeterte øvelser, 2. På problem aktiviteter, 3. Standardiserte oppgaver, 4. Spesifikke kognitive domener (Gates, 2010). Ulike typer: Adaptiv vs. Strategi trening
. Ulike typer: Adaptiv vs. Strategi trening.")
3
Mange måter å gjøre det på!

4
LONDON

5
Drosjesjåfører

6
Sjonglering! In the study of juggling training, a significant expansion in grey matter was found both bilaterally and posterior on the left side, and the yellow areas represents the change in grey matter. Endringer I grå substans I hjernen (økt volum) etter at man hadde trent på å sjonglere. Draganski B et al. Nature 2004; 427:311
 etter at man hadde trent på å sjonglere. Draganski B et al. Nature 2004; 427:311.")
7
Grunnlag for intervensjon
Plastisitet Kapasiteten til å modifisere hjernestruktur og funksjon. Resiliens Sparte funksjoner Utkomme påvirkes av andre faktorer enn skaden This will include social factors, like poverty, as well as access to medical and educational resouces. Sosiale faktorer Tilgang til ressurser innen helse og utdanning Spevack, 2007: Pediatric Neuropsychological interventions. Taylor, et.al. 2010; Anderson et.al., 2011)
")
8
Hvordan modifisere hjerneskader/dysfunksjon?
Primært Medisinsk Reparere/minimere skaden Primary interventions to stop and reduce the consequences of brain injury would be the medical interventions done at the Neonatal Intensive Care Unit.

9
Hvordan modifisere hjerneskader/dysfunksjon?
Primært Medisinsk Reparere/minimere skaden Sekundære Redusere funksjonelle konsekvenser Primary interventions to stop and reduce the consequences of brain injury would be the medical interventions done at the Neonatal Intensive Care Unit.

10
Hvordan modifisere hjerneskader/dysfunksjon?
Primært Medisinsk Reparere/minimere skaden Sekundære Redusere funksjonelle konsekvenser Primary interventions to stop and reduce the consequences of brain injury would be the medical interventions done at the Neonatal Intensive Care Unit. Tertiære Kompensere Bedre utkomme

11
Hvordan vite om det virker?
Forskningsmessig er vi oopptatt av mekanismer Endringer i kjemi /energi (dopamin, funksjonell MRI) Endringer i struktur (kvantitativ MRI) Grå substans Hvit substans Klinisk er vi opptatt av funksjonsendring Bedret funksjon
 Endringer i struktur (kvantitativ MRI) Grå substans. Hvit substans. Klinisk er vi opptatt av funksjonsendring. Bedret funksjon.")
12
Hovedutfordring med kognitiv trening:
Overføring! – treningseffekt på oppgaver du ikke har trent på. Begrenset Type trening er avgjørende K X B G S M Green & Bavalier, 2008

13
Sikte mot overføringseffekt – mekanismer.
Delte nettverk (Jaeggi, 2008). Trening som aktiverer høyere ordens kognisjons områder I hjernen (Klingberg, 2010; Olesen, 2003) Recent research indicates that transfer effects between functions may be expected if there is a shared underlying neural network. If the training is targeted to functions carried out by higher association cortices – this may promote transfer.
. Trening som aktiverer høyere ordens kognisjons områder I hjernen (Klingberg, 2010; Olesen, 2003) Recent research indicates that transfer effects between functions may be expected if there is a shared underlying neural network. If the training is targeted to functions carried out by higher association cortices – this may promote transfer.")
14
Oppmerksomhet og eksekutive funksjoner – Hjernens direktør
Primært anatomisk korrelat - frontallappen Trolig ikke ferdig modnet før ung voksen alder: Forsinket myelinisering (Giedd, 1999) Tynning av cortex - beskjæring (nevroner – grå substans) fortsetter gjennom ungdomsårene? Mechanism not clearly established (Webster, 2010) Responsibility for such ”higher order cognitive functions” is primarily in the prefrontal cortex. This is the last part of our brain do develop, and myelination continue through young adulthood. In addition, an extensive pruning of synapses are thought to take place throughout adolescents.
 Tynning av cortex - beskjæring (nevroner – grå substans) fortsetter gjennom ungdomsårene Mechanism not clearly established (Webster, 2010) Responsibility for such higher order cognitive functions is primarily in the prefrontal cortex. This is the last part of our brain do develop, and myelination continue through young adulthood. In addition, an extensive pruning of synapses are thought to take place throughout adolescents.")
15
Oppmerksomhet og eksekutive funksjoner
“Damage to any link in the complex system underlying executive functions can result in functional deficits” (Anderson, 2010) These functions are relying on an extensive connectivity to other parts of the brain. Damage to any link in this complex systems underlying these functions can result in deficits. Held together with our knowledge that brain injury in preterms may affect both cortical and subcortical structures, as well as white matter – it makes sense that these functions are often reported as reduced in preterm groups. Hvit-substans banene I hjernen Oishi, 2010
 These functions are relying on an extensive connectivity to other parts of the brain. Damage to any link in this complex systems underlying these functions can result in deficits. Held together with our knowledge that brain injury in preterms may affect both cortical and subcortical structures, as well as white matter – it makes sense that these functions are often reported as reduced in preterm groups. Hvit-substans. banene I. hjernen. Oishi,")
16
Attention/executive functions – intertwined
On the positive side, this reliance on a multiplicity of brain areas and connections makes attention executive functions a good target for cognitive training. This figure illustrates central elements of attention/executive functions:

17
Attention/executive functions - intertwined
As this figure illustrates nicely, these abilities are intertwined, meaning that if you modify one of them, the chance is that you also affect the others.

18
Attention/executive functions - intertwined
As this figure illustrates nicely, these abilities are intertwined, meaning that if you modify one of them, the chance is that you also affect the others.

19
Hva er arbeidsminne? evne til å holde informasjon «online» mens vi samtidig arbeider med den. Eks. Hoderegning Lytte til forelesning Ta imot beskjeder

20
Tegn på vansker med arbeidsminne
Problemer med å holde fokus på det du skal. Lett å distrahere Problemer med å komme i gang med og med å fullføre oppgaver Problemer med å huske instruksjoner Avbryter ofte (vansker med å vente på tur) Vansker med å organisere seg / arbeidet sitt Lærevansker (lesing, matte og trekke ut essensen av det du hører/leser, få med seg muntlig informasjon)
 Vansker med å organisere seg / arbeidet sitt. Lærevansker (lesing, matte og trekke ut essensen av det du hører/leser, få med seg muntlig informasjon)")
21
Arbeidsminne og konsentrasjon
Barn som strever med konsentrasjon (inkludert barn med ADD/ADHD) har ofte også problemer med arbeidsminne.
 har ofte også problemer med arbeidsminne.")
22
Bedring av arbeidsminne funksjon etter trening har blitt vist hos:
Friske voksne (Olesen, et.al. 2003) Friske ungdommer (Løhaugen, et.al. 2010) Kliniske grupper: Barn med ADHD ADHD (Klingberg, et.al. 2002; 2005) Voksne 1-3 år etter slag (Westerberg, et.al. 2007) Voksne med traumatisk hjerneskade (Serino et.al. 2007). Ungdommer med ekstremt lav fødselsvekt (Løhaugen et.al. 2010) Ulike metoder – alle gav overføringseffekt Improvements in working memory after training has been demonstrated in healthy adults, children with ADHD, in stroke patients, after traumatic brain injury and in extremely low birth weight adolescents. The methods used in these studies varied somewhat, but there were transfer effects to non-trained tasks, that is tasks that assesses the same function but not by the same type of task. I`ll show you an example from the stroke study to illustrate the type of training as well as results.
 Friske ungdommer (Løhaugen, et.al. 2010) Kliniske grupper: Barn med ADHD ADHD (Klingberg, et.al. 2002; 2005) Voksne 1-3 år etter slag (Westerberg, et.al. 2007) Voksne med traumatisk hjerneskade (Serino et.al. 2007). Ungdommer med ekstremt lav fødselsvekt (Løhaugen et.al. 2010) Ulike metoder – alle gav overføringseffekt. Improvements in working memory after training has been demonstrated in healthy adults, children with ADHD, in stroke patients, after traumatic brain injury and in extremely low birth weight adolescents. The methods used in these studies varied somewhat, but there were transfer effects to non-trained tasks, that is tasks that assesses the same function but not by the same type of task. I`ll show you an example from the stroke study to illustrate the type of training as well as results.")
23
Treningsprogram Det finnes mange ulike treningsprogram
Praktiske «skole-liknende» program PC-programmer Noen forskes det på og andre ikke Noen kan kjøpes fritt og andre må man ha oppfølging under.

24
J Pediatr. 2011 Apr;158(4):555-561.e4.Epub 2010 Dec 3.
I will present to you our results from the paper ”Computerized working memory training improves function in adolescents born at extremely low birth weight” that was published in Journal of Pediatrics in 2011. J Pediatr Apr;158(4): e4.Epub 2010 Dec 3.
: e4.Epub 2010 Dec 3.")
25
Mål for undersøkelsen:
Å evaluere om databasert arbeidsminnetrening kunne bedre arbeidsminne hos ungdom født med ekstremt lav fødseslvekt (under 1000 gram) uavhengig av tilleggsvansker (eks. CP) og forståelsesvansker (lærevansker) Vi ønsket å se på effekten I forhold til oppgaver de hadde trenet på og overføringsverdi til andre områder. Vi ønsket å se om effekten varte over tid. Effect of computerized working memory training in ELBW adolescents? Generalized effect? Lasting effect? The aim was to evaluate if a computerized WM training program (Cogmed RM) developed for children with ADHD could improve working memory in ELBW adolescents regardless of low IQ and additional impairments. We also wanted to examine if a beneficial effect would generalize to other memory functions, indicating a positive effect on learning ability. Lastly we examined if there was a lasting effect of training, and whether there would be any differences in the long term effect between the ELBW group and controls
 uavhengig av tilleggsvansker (eks. CP) og forståelsesvansker (lærevansker) Vi ønsket å se på effekten I forhold til oppgaver de hadde trenet på og overføringsverdi til andre områder. Vi ønsket å se om effekten varte over tid. Effect of computerized working. memory training in ELBW adolescents Generalized effect Lasting effect The aim was to evaluate if a computerized WM training program (Cogmed RM) developed for children with ADHD could improve working memory in ELBW adolescents regardless of low IQ and additional impairments. We also wanted to examine if a beneficial effect would generalize to other memory functions, indicating a positive effect on learning ability. Lastly we examined if there was a lasting effect of training, and whether there would be any differences in the long term effect between the ELBW group and controls.")
26
Treningsprogrammet vi har brukt:
Cogmed RM® computer program, (Cogmed Cognitive Medical Systems AB, Stockholm). 35-50 minutter daglig, 5 dager uken, i 5 uker. Coaching en gang i uken fra psykolog ansatt i Cogmed. The intervention program consisted of performing WM tasks in the Cogmed RM program. This was bought from the Cogmed Cooperation and provided for free to the participants. All participants received a CD with the program, and used it at home for minutes a day, five days a week for a five-week period. Once a week the family received a telephone call from a trained psychologist working at CogMed that provided feedback and motivational support based on the result from the last five training days.
 minutter daglig, 5 dager uken, i 5 uker. Coaching en gang i uken fra psykolog ansatt i Cogmed. The intervention program consisted of performing WM tasks in the Cogmed RM program. This was bought from the Cogmed Cooperation and provided for free to the participants. All participants received a CD with the program, and used it at home for minutes a day, five days a week for a five-week period. Once a week the family received a telephone call from a trained psychologist working at CogMed that provided feedback and motivational support based on the result from the last five training days.")
28
Login

29
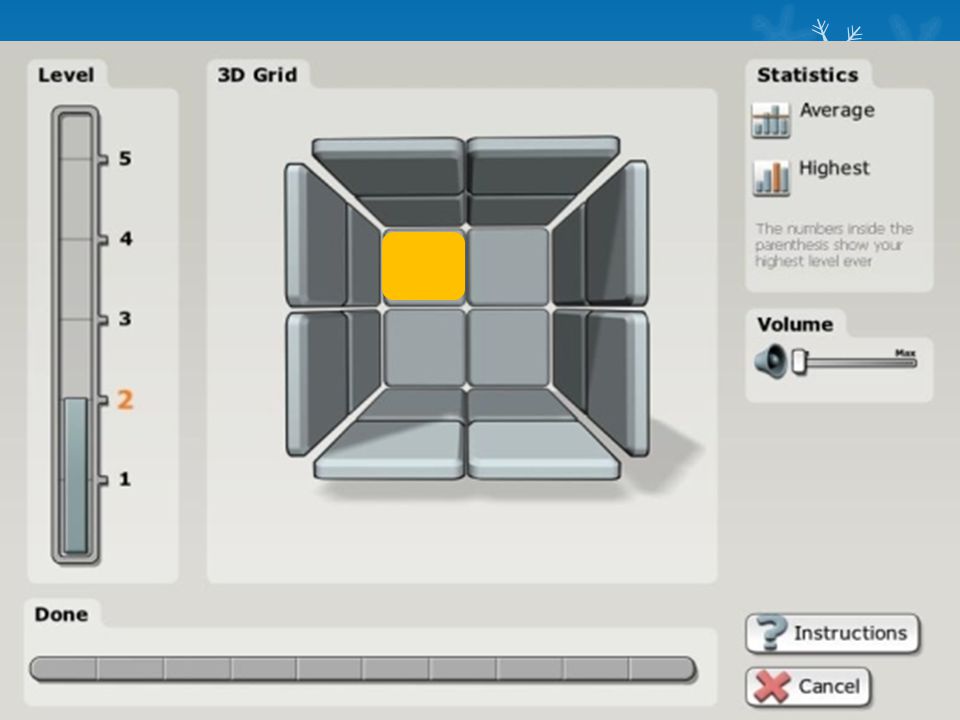
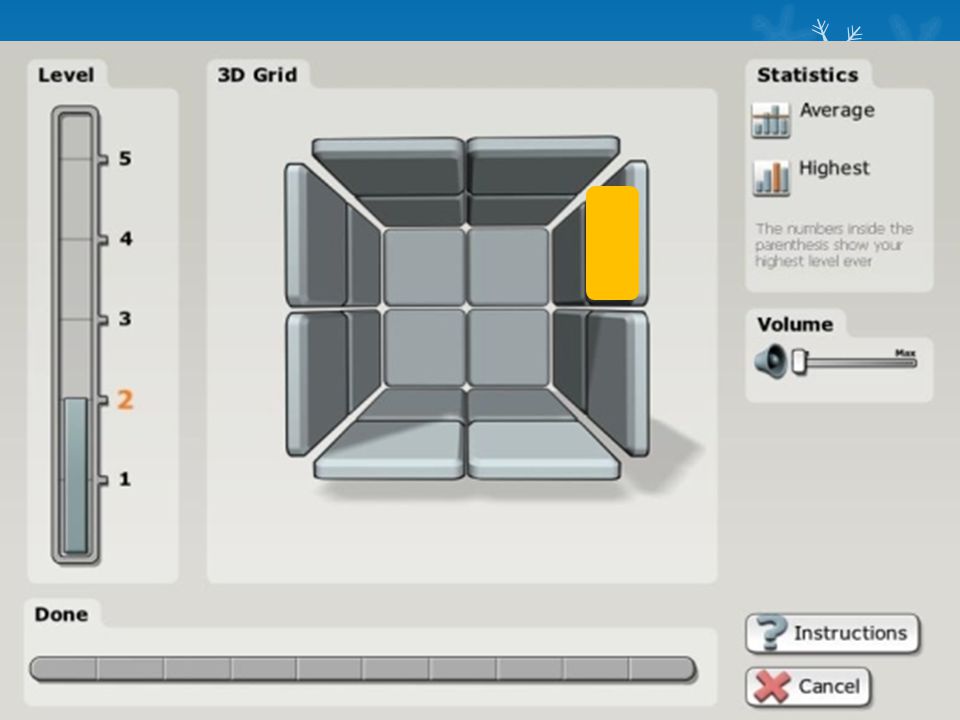
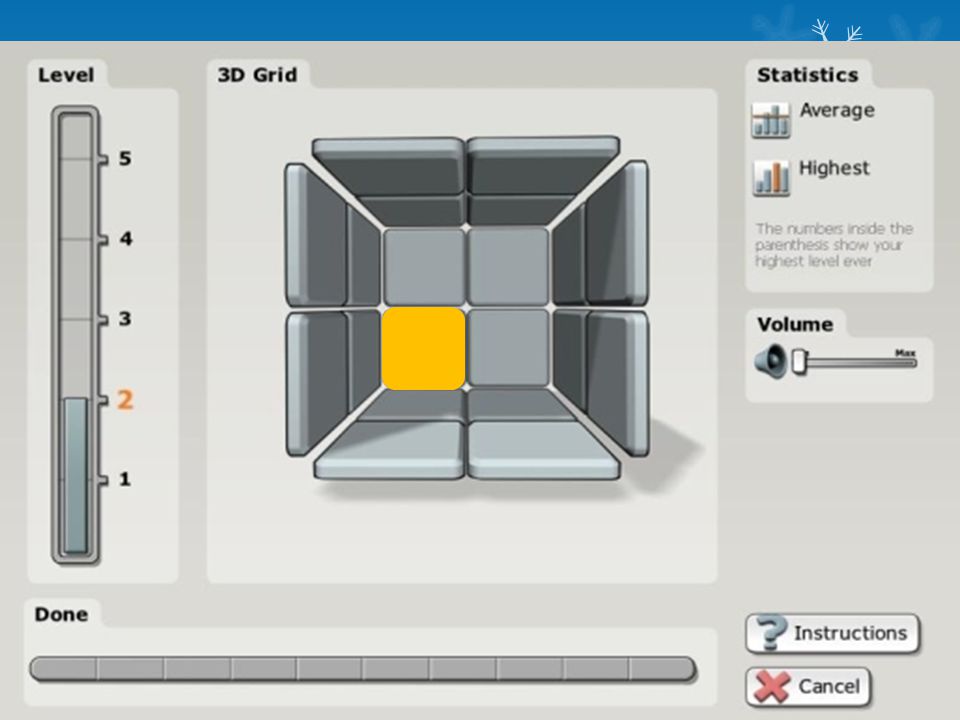
The Cogmed RM program resembles a video game, but is comprised of several different “games” that require visuo-spatial WM, for example remembering the position of objects, as well as a combination of verbal and visual WM , like remembering phonemes, letters and digits. The difficulty level for each task was adjusted automatically and continuously as the child improved during each session. This is what greets the user when the program is started. The robot and all the different tasks to be done.They can be started by clicking on them, and you may choose the order in which they are done. On the right is an example of one task where the child is to remember what letters light up and in which order to repeat it after the robot. As you work through the program you also collect fuel for a revard racing game at the end of the session, and the energy bar on the right side of the screen shows how much energy you have collected.

30
Visuell data link

31
Arbeidsminnetrening for førskolebarn
10-15 min daglig 5 dager I uken 5 uker The children trained with the Cogmed JM program that is designed for pre-school aged children. The program is based solely on visual-spatial stimuli and consists of 7 different rotating tasks. On the computer screen the child is presented to pictures like this, where fur balls jump up in a certain order. The child must remember the sequence and then click on the fur balls in the same order. The JM software increases the difficulty level in real time, as the child’s skills improve. The children were training minutes a day, 5 days a week for 5 weeks, that is 25 training sessions. Images with permission Cogmed JM

32
Voksenversjon

33
Now you try to remember. Not so easy
Now you try to remember. Not so easy. After this, the program would say ”well done”.

38
Now you try to remember. Not so easy
Now you try to remember. Not so easy. After this, the program would say ”well done”.

39
Now you try to remember. Not so easy
Now you try to remember. Not so easy. After this, the program would say ”well done”.

40
Ungdom med fødselsvekt under 100gram og kontroller som var terminfødte.
ELBW Mean (sd) Controls P-value N=16 N=19 Birth weight (grams) 778 (118) 3924 (528) <0.001 Gestational age (weeks) 25.8 (1.8) - Socio-economic status 3.1 (1.2) 3.7 (1.3) 0.282 IQ (WISC-III) 78 (13) 100 (12) <0.01 Age at assessment 14.1 (0.6) 14.3 (0.7) 0.314 In this intervention study all 34 ELBW adolescents born in 1992 and 1993 were offered to participate. 53% consented, and 16 of the 18 ELBW children fulfilled the training. We had 11 girls and only 5 boys in the ELBW group. 19 term born controls were also included, 6 females and 13 males. In addition, 11 controls were included that did not train to assess the effect of repeating working memory tasks on test results. In addition 11 controls were included to assess the test-retest effect on working memory for different neuropsychological tests.
 Controls. P-value. N=16. N=19. Birth weight (grams) 778 (118) 3924 (528) < Gestational age (weeks) 25.8 (1.8) - Socio-economic status. 3.1 (1.2) 3.7 (1.3) IQ (WISC-III) 78 (13) 100 (12) <0.01. Age at assessment (0.6) 14.3 (0.7) In this intervention study all 34 ELBW adolescents born in 1992 and 1993 were offered to participate. 53% consented, and 16 of the 18 ELBW children fulfilled the training. We had 11 girls and only 5 boys in the ELBW group. 19 term born controls were also included, 6 females and 13 males. In addition, 11 controls were included that did not train to assess the effect of repeating working memory tasks on test results. In addition 11 controls were included to assess the test-retest effect on working memory for different neuropsychological tests.")
41
Resultat før og etter trening på oppgavene fra programmet
These are results from the trained working memory tasks provided from the Cogmed program. The ELBW group scored significantly lower than the control group on the Start Index in the program.

42
However, after training there were no significant differences between groups on Max Index or on the Improvement Index

43
Effekt på oppgaver som ikke var med I programmet – overføringseffekt av trening til andre funksjoner. Marked in green are the results immediately after the training, and you can see that the ELBW group improved significantly on four of the seven tasks, and the controls improved on three of the tasks.

44
Effekt etter 6 mnd After 6 moths the ELBW group still showed results significantly better than before training, but no further improvement. The controls had continued to improve significantly after training. We have speculated if this reflects that the ELBW group experiences a “boster” effect from the trainng, and then returns to a somewhat slower slope of development than the controls that continues developement at expected pace.

45
Vi lurte på om det bare var de som ikke hadde lærevansker
Som ble bedre – og delte gruppen for å se på dette. In both groups there was a significant improvement on a majority of these tasks, marked in green.

46
Ble de bedre fordi de repeterte tester?
Both ELBW and control participants improved their baseline scores on tests measuring non-trained visual and verbal WM from baseline to immediately after training, illustrated here by total raw scores on the digit span task. The blue line are the ELBW group, while the green represents the controls. After training the ELBW group still scores lower than controls, but their result are now well within where the controls started our, maybee indicating a nomalization of working memory capasity after training. The flat, black line shows that there were no significant differences in raw scores in the non-trained control group after the test-retest of working memory. This indicates that repeating working memory tasks does not result in a significant practice effect.

47
Konklusjoner Ungdommer født med ELBW ble bedre både på på oppgavene de trente på og andre oppgaver som krever arbeidsminne Ungdom med lav IQ (<80) og/eller CP ble også signifikant bedre. Treningen førte til like mye endring i både prematur og kontroll gruppen. Vi så overføringseffekt til verbal læring i ELBW gruppen, noe som er svært viktig for skoleprestasjoner. Resultatene holdt seg stabile over 6 mnd i prematur gruppen. To conclude: Our main finding was that a group of ELBW children improved trained and non-trained working memory results after participation in the Cogmed RM training program. ELBW individuals with low IQ (<80) benefitted significantly from the training and the program had similar effect in those with normal and subnormal or low IQ. The results remained relatively stable in the ELBW group over time.
 og/eller CP ble også signifikant bedre. Treningen førte til like mye endring i både prematur og kontroll gruppen. Vi så overføringseffekt til verbal læring i ELBW gruppen, noe som er svært viktig for skoleprestasjoner. Resultatene holdt seg stabile over 6 mnd i prematur gruppen. To conclude: Our main finding was that a group of ELBW children improved trained and non-trained working memory results after participation in the Cogmed RM training program. ELBW individuals with low IQ (<80) benefitted significantly from the training and the program had similar effect in those with normal and subnormal or low IQ. The results remained relatively stable in the ELBW group over time.")
48
MEN! Da begynte vi å lure på noe mer fordi:
De som hadde cerebral parese hadde særlig god effekt Men bare 3 barn! Hvordan finne ut om det faktisk er slik at barn med CP har særlig nytte av arbeidsminnetrening? Større studie = flere barn

49
Arbeidsminnetrening for barn med CP – et multi-senter studie Innvilget støtte fra extra stiftelsen og søkt via CP-foreningen

50
Multi-senter studie som ledes fra HABU-Arendal
Vestfold /CP registeret (Phd Guro Andersen) Telemark (Phd Gro Løhaugen, spesfys. Cato Sundberg) Rogaland (Phd Harald Beneventi) Nord- og Sør-Trøndelag (Professor Jon Skranes, Professor Torstein Vik, Psykolog Heidi Furre Østgård) Aust- og Vest-Agder: HABU-Arendal (Spes.fysioterpeut Cato Sundberg og Phd Gro Løhaugen) MÅL: 115 barn med CP gjennomfører arbeidsminnetrening. 64 barn har startet opp, noen har falt fra (ca 5).
 Telemark (Phd Gro Løhaugen, spesfys. Cato Sundberg) Rogaland (Phd Harald Beneventi) Nord- og Sør-Trøndelag (Professor Jon Skranes, Professor Torstein Vik, Psykolog Heidi Furre Østgård) Aust- og Vest-Agder: HABU-Arendal (Spes.fysioterpeut Cato Sundberg og Phd Gro Løhaugen) MÅL: 115 barn med CP gjennomfører arbeidsminnetrening. 64 barn har startet opp, noen har falt fra (ca 5).")
51
Utfordringer ved å forske på effekt av kognitiv trening:

52
Placebo effekt Trening = positiv oppmerksomhet, forventning om effekt fra foreldre, barn og forskeren

53
”Blindet” Den som forsker bør ikke vite hvem som får hvilken behandling! Utfordring ved forskning i klinikk Mulig løsning: samarbeid på tvers av tjenester?

54
Stepped Wedge Design = kostbart og tidkrevende
Slide fra Overlege og Phd stipendiat Kristine Hermansen Grunewaldt, NTNU, 2012.

55
Praktisk 1. Barna møter i nærheten av hjemmet (habu, hotell, skole) før trening for å gjennomgå oppgaver (2-3 timer) Foreldrene svarer på spørsmål om dagliglivets funksjon, arbeidsminne, oppmerksomhet etc i form av spørreskjema Etter første avtale får familien beskjed om de skal starte trening umiddelbart eller vente til etter neste kontroll (10 uker senere) 2. Ny kontroll på samme sted ca 10 uker senere (ca 1 time) Trening eller venting 10 uker 3. Ny kontroll på samme sted 4. Kontroll 6 mnd etter ferdig trening
 2. Ny kontroll på samme sted ca 10 uker senere (ca 1 time) Trening eller venting 10 uker. 3. Ny kontroll på samme sted. 4. Kontroll 6 mnd etter ferdig trening.")
56
Oppfølging under treningen
Telefon fra en «trener» 1 gang per uke Samtale om hvordan treningen går Tips i forhold til å få mer ut av treningen og i forhold til motivasjon. Noen ganger snakker coachen med både barn og foreldrene, i andre tilfeller bare med foreldrene ( min pr uke).
.")
57
Coaching

58
Hvem kan være med? Barn med CP mellom 6 og 15 år
Alle typer CP men må kunne bruke datamus Ikke fotosensistiv epilepsi NB! Oslo/Akershus får invitasjoner I Februar/Mars – via CP- registeret;)
")
59
Ønsker dere å være med eller få vite mer – vet dere om noen som kan ha nytte av dette?
Ved spørsmål kan dere kontakte Cato Sundberg eller Gro Løhaugen på telefon (HABU-A) Gro Løhaugen: Eller mail:
 Gro Løhaugen: Eller mail:")
60
Based on what we now know – what can be done to improve the chances of such interventions having a transfer effect in preterm adolescents and young adults? As this is a vulnerable group and cost effectiveness will be important to evaluate. Hva kan vi gjøre for å bedre sjansen for et godt resultat etter kognitiv trening – uansett type?

61
Viktige prinsipper: ”Zone of proximal development” (Vygotsky, 1978)
“If One Is Truly to Succeed in Leading a Person to a Specific Place, One Must First and Foremost Take Care to Find Him Where He is and Begin There. This is the secret in the entire art of helping”. Søren Kierkegaard. Studies on learning and training of lost functions has been well established in both experimental psychology and in rehabilitation. The challenge is to obtain a transfer effect to other than the trained skill. To improve outcome of training there are several factors that are important. Maybe the most important principle is to remember what Vygotsky called the zone of proximal development. The Danish philosopher Kirkegaard described this beautifully : If One Is Truly to Succeed in Leading a Person to a Specific Place, One Must First and Foremost Take Care to Find Him Where He is and Begin There. This is the secret in the entire art of helping. Tranferred to neuropsychological rehablitation, individual assessment of function is necessary to plan interventions.

62
Når vi sikter etter overføring til andre funksjoner enn dem man trener – hva vet vi er viktig da?
Vanskelighetsgrad på oppgavene (realistiske) (Green, 2008; Jaeggi, 2011) Oppgavene tilpasses (gradvis økt belastning) (Jansma, 2001; Klingberg, 2002; Klingberg 2005) Motivasjon (Green, 2008; Jaeggi, 2011) Tilbakemelding (feedback) (Jaeggi, 2011, Green, 2008) Varighet (Klingberg, 2002; 2005; Holmes, 2009; Jaeggi, 2008) This will enable the intervention to be at the correct level of difficulty for the individual. This is important based on cognitive training studies showing that if the participant experiences the task as to hard, the effect i lower, as demonstrated by Jaeggi in a recent study. Also, the intervention should be dynamic in its form – adjusting the level of demand as the person improves. Realistic adjustment of demand also affects motivation positively. Feedback on progress improves outcome and should be planned for, and any intervention should be carried out over some time. This applies for cognitive training, but also to interventions of a more compensatory type. To sum up: The task to be trained should be just a little harder than what you already are able to perform. Learning and motivation will be at its maximum when the task represents a challenge – but still feels doable.
 (Green, 2008; Jaeggi, 2011) Oppgavene tilpasses (gradvis økt belastning) (Jansma, 2001; Klingberg, 2002; Klingberg 2005) Motivasjon (Green, 2008; Jaeggi, 2011) Tilbakemelding (feedback) (Jaeggi, 2011, Green, 2008) Varighet (Klingberg, 2002; 2005; Holmes, 2009; Jaeggi, 2008) This will enable the intervention to be at the correct level of difficulty for the individual. This is important based on cognitive training studies showing that if the participant experiences the task as to hard, the effect i lower, as demonstrated by Jaeggi in a recent study. Also, the intervention should be dynamic in its form – adjusting the level of demand as the person improves. Realistic adjustment of demand also affects motivation positively. Feedback on progress improves outcome and should be planned for, and any intervention should be carried out over some time. This applies for cognitive training, but also to interventions of a more compensatory type. To sum up: The task to be trained should be just a little harder than what you already are able to perform. Learning and motivation will be at its maximum when the task represents a challenge – but still feels doable.")
63
The brain is wider than the sky, For, put them side by side, The one the other will contain With ease, and you beside.

Liknende presentasjoner