Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Traumepasienten - prioriteres luftvei før columnaskade?

2
Traumepasienten – prioriteres luftvei før columnaskade?
Per Kristian Hyldmo PhD-stipendiat, SNLA og UiS og overlege, luftambulanse, Sørlandet sykehus HF ALNSF Fagkongress 2013, Arendal Lærer A dreper fortere enn B enn C enn D - men er det alltid sånn i praksis.?

3
En vakker fredags natt i Akuttmottak…
Mann, 24, trafikkulykke: Stroppet fast på ryggbrett Kjevegrep, O2, SpO2 92% God pulsfylde, p 78 Bevisstløs, GCS 6 Blod fra nese Intubasjon: Blod og litt mageinnhold, ellers ua. 40 min. siden ulykka Håndsopprekning: noen som har opplevd en slik pasient..?

4
Blir A prioritert før D…?
Han kan ha nakke-/ryggskade.. Våken pas. med symptomer: OK å ”begrense spinal bevegelse”

5
Blir A prioritert før D…?
Men dette er ikke å prioritere A før D Løsning…?

6
En pasient til Håndverker i nybygg, fall fra 2. etg. betonggulv
Amb. framme: På ny bevisstløs O2, nakkekrage, Traumesideleie, startet transport 45 min senere: Bevisstløs, SpO2 94 %, intubert i amb. Sug: Litt blod ++ fra innsiden av kinn Laryngoskopi: Ikke blod nær stemmespalten Sug fra tube: Intet ETCO2 ca 8 etter intubasjon

7
Utgangspunkt Bevisstløs, skadet pasient… Hodeskade tåler IKKE:
hypoksi hypo- eller hyperventilering BT-fall Men han KAN ha nakke-/ryggskade…?

8
Forutsetninger og antakelser
Det er farlig å ligge på ryggen Sideleie ”sikrer” luftveier Det er trygt å log-rolle pasient = Traumesideleie

9
Traumesideleie

10
Traumesideleie

11
Traumesideleie

12
Traumesideleie

13
Traumesideleie

14
Traumesideleie

15
Traumesideleie

16
Traumesideleie

17
Traumesideleie Håndsopprekning? Noen som har sett pas. komme inn på denne måten?

18
Brukes Traumesideleie i Norge?
Of 206 ground EMS supervisors, 201 answered; 75% reported that LTP is used. In services using LTP, written protocols were present in 67% and 73% had provided training in LTP use. Questionnaires were distributed to 3,025 ground EMS personnel. We received 1,395 (46%) valid questionnaires. LTP was known to 89% of respondents, but only 59% stated that they use it. Of the respondents using LTP, 77% reported access to written protocols. Flexing of the top knee was reported by 78%, 20% flexed the bottom knee, 81% used under head padding. Of 24 air EMS supervisors, 23 participated. LTP is used by 52% of the services, one of these has a written protocol and three arrange training.
 valid questionnaires. LTP was known to 89% of respondents, but only 59% stated that they use it. Of the respondents using LTP, 77% reported access to written protocols. Flexing of the top knee was reported by 78%, 20% flexed the bottom knee, 81% used under head padding. Of 24 air EMS supervisors, 23 participated. LTP is used by 52% of the services, one of these has a written protocol and three arrange training.")
19
Spørsmål som trenger svar
ER det farlig å ligge på ryggen når en er bevisstløs…? Gitt en ustabil nakkeskade, er det farlig å snu på siden? Hvor mange skadde, bevisstløse pasienter har samtidig en nakke-ryggskade? Hva skjer med ustabilt nakkebrudd ved Stabilt sideleie eller HAINES? Traumesideleie?

20
ER det farlig å ligge på ryggen når en er bevisstløs…?
Vet vi ikke det fra før…? Systematisk oversikt på gang: Studier på søvnapne Barn i narkose Slagpasienter

21
Gitt en ustabil nakkeskade, er det farlig å snu på siden?
5-year retrospective chart review 2 university hospitals. All patients with acute blunt traumatic spinal or spinal cord injuries transported directly from the injury site to the hospital None of the 120 patients seen at the University of Malaya had spinal immobilization during transport all 334 patients seen at the University of New Mexico did. The 2 hospitals were comparable in physician training and clinical resources. There was less neurologic disability in the unimmobilized Malaysian patients (OR 2.03; 95% CI ; p = 0.04). This corresponds to a ~ 2 c%hance that immobilization has any beneficial effect. Results were similar when the analysis was limited to patients with cervical injuries (OR 1.52; 95% CI ; p = 0.34).
. This corresponds to a ~ 2 c%hance that immobilization has any beneficial effect. Results were similar when the analysis was limited to patients with cervical injuries (OR 1.52; 95% CI ; p. = 0.34).")
22
Gitt en ustabil nakkeskade, er det farlig å snu på siden?
Hauswald 1998 (rygg- og nakkeskader): Mindre nevrologisk skade i Malaysia (OR 2.03; 95% CI ; p = 0.04) Nakkeskader alene: (OR 1.52; 95% CI ; p = 0.34). Kuala Lumpur:” None of the ED staff could remember any patients who had been immobilized..”
: Mindre nevrologisk skade i Malaysia (OR 2.03; 95% CI ; p = 0.04) Nakkeskader alene: (OR 1.52; 95% CI ; p = 0.34). Kuala Lumpur: None of the ED staff could remember any patients who had been immobilized..")
23
Gitt en ustabil nakkeskade, er det farlig å snu på siden?
Systematisk oversikt: Finner ingen litteratur på nevrologisk forverring som utfallsmål Div kadaverstudier: Viser betydelig bevegelse ved log-roll Men hvor mye bevegelse er farlig??

24
Hvor mange skadde, bevisstløse pasienter har samtidig en nakke-ryggskade?
Hvor mange skadde, bevisstløse pasienter har samtidig nakke-ryggskade? 5-10%?? Kan gi grunnlag for å veie den ene risikoen mot den andre Planlagt studie i SUS’ traumedatabase (og evt. OUS’)
")
25
Hva skjer med ustabilt nakkebrudd ved Traumesideleie?

26
University of Florida

27
Hva skjer med ustabilt nakkebrudd ved Traumesideleie?
Forbausende liten forskjell på stabilt sideleie, HAINES og traumesideleie Ny studie: Log-roll vs. Traumesideleie

28
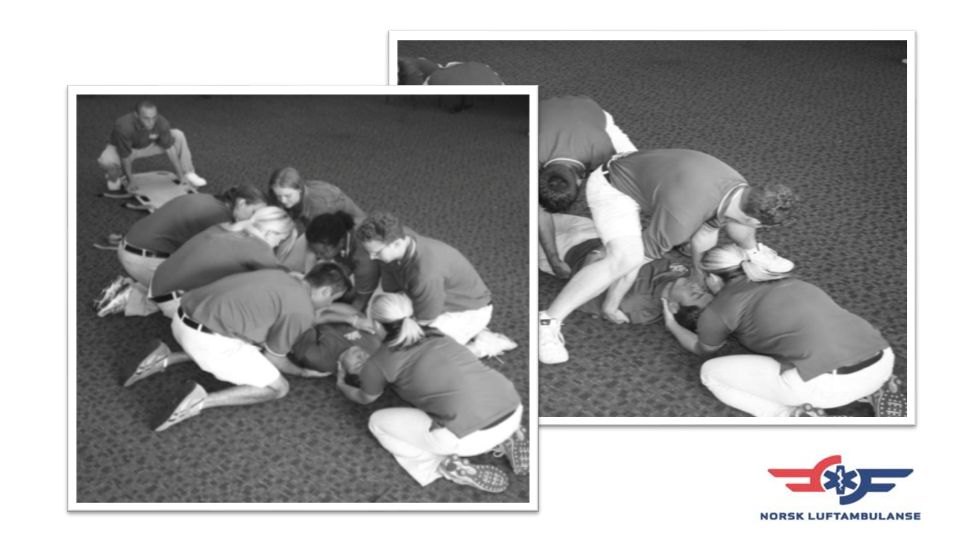
Er log-roll ufarlig?

29
Σ Oppsummert så langt: Det er farlig å ligge bevisstløs på ryggen?
Lite evidens om hvor farlig det er å snu over på siden Log-roll gir betydelig bevegelse i ustabil columna-fraktur

30
Bedre enn log-roll The execution of the LR maneuver tends to generate more motion than either of the lifting methods examined in this investigation.

32
Bedre enn log-roll The effectiveness of the scoop stretcher to limit spinal motion in the destabilized spine is comparable or better than manual techniques currently being used by primary responders.

33
Er nakkekrage god behandling?

34
Er nakkekrage god behandling?
Antakelser, jfr. Benger & Co: Skadde kan ha en ustabil nakke Bevegelse kan forverre skaden Nakkekrage beskytter mot bevegelse Nakkekrage er ufarlig, og dermed trygt for de fleste pasienter Kollega Helge Asbjørnsen, HUS: Sammendrag i Update

35
Er nakkekrage god behandling?
Falsk trygghet? Canadian C-spine rule Stor prehospital studie pågår Ikke til penetrerende skader (ingen immobilisering)
")
36
Xcollar – ny krage Stabiliserer bedre? Trenger ikke nøytralstilling
Komplisert å sette på OBS! Hakestropp og luftveier Fare for stor traksjon?

37
Ryggbrett kan ha en pris…
BMJ 2004 Aug 28;329(7464):495-9. Morris et al: Spinal immobilisation for unconscious patients with multiple injuries.
: Morris et al: Spinal immobilisation for unconscious patients with multiple injuries.")
38
“… Once extricated, patients should be taken off the backboard.”
Connecticut viser vei? “… Once extricated, patients should be taken off the backboard.” Connecticut Emergency Medical Services Medical Advisory Committee (CEMSMAC) National Association of EMS Physicians Position Statement Backboards The National Association of EMS Physicians Believes That: • There is no evidence that the use of a backboards reduces spinal injury or effectively
provides anatomically appropriate spinal immobilization or protection. • There is evidence that backboards result in harm by causing pain, changing the normal anatomic lordosis of the spine, inducing patient agitation, causing pressure ulcers, and compromising respiratory function. • The only practical value of backboards is for extrication to a transport vehicle. Once
extricated, patients should be taken off the backboard. • Backboards should not be used for spinal immobilization. Placing ambulatory patients
on backboards is unacceptable. • In general, patients should not be transported or otherwise kept on backboards for any
length of time.
 National Association of EMS Physicians Position Statement Backboards. The National Association of EMS Physicians Believes That: • There is no evidence that the use of a backboards reduces spinal injury or effectively provides anatomically appropriate spinal immobilization or protection. • There is evidence that backboards result in harm by causing pain, changing the normal anatomic lordosis of the spine, inducing patient agitation, causing pressure ulcers, and compromising respiratory function. • The only practical value of backboards is for extrication to a transport vehicle. Once extricated, patients should be taken off the backboard. • Backboards should not be used for spinal immobilization. Placing ambulatory patients on backboards is unacceptable. • In general, patients should not be transported or otherwise kept on backboards for any length of time.")
39
“Backboards should not be used for spinal immobilization”
Connecticut viser vei? “Backboards should not be used for spinal immobilization” Connecticut Emergency Medical Services Medical Advisory Committee (CEMSMAC) National Association of EMS Physicians Position Statement Backboards The National Association of EMS Physicians Believes That: • There is no evidence that the use of a backboards reduces spinal injury or effectively
provides anatomically appropriate spinal immobilization or protection. • There is evidence that backboards result in harm by causing pain, changing the normal anatomic lordosis of the spine, inducing patient agitation, causing pressure ulcers, and compromising respiratory function. • The only practical value of backboards is for extrication to a transport vehicle. Once
extricated, patients should be taken off the backboard. • Backboards should not be used for spinal immobilization. Placing ambulatory patients
on backboards is unacceptable. • In general, patients should not be transported or otherwise kept on backboards for any
length of time.
 National Association of EMS Physicians Position Statement Backboards. The National Association of EMS Physicians Believes That: • There is no evidence that the use of a backboards reduces spinal injury or effectively provides anatomically appropriate spinal immobilization or protection. • There is evidence that backboards result in harm by causing pain, changing the normal anatomic lordosis of the spine, inducing patient agitation, causing pressure ulcers, and compromising respiratory function. • The only practical value of backboards is for extrication to a transport vehicle. Once extricated, patients should be taken off the backboard. • Backboards should not be used for spinal immobilization. Placing ambulatory patients on backboards is unacceptable. • In general, patients should not be transported or otherwise kept on backboards for any length of time.")
40
Transport på denne?

41
Ikke transporter på ryggbrett,
X Ikke transporter på ryggbrett, bruk vakuummadrass!

42
Bruk Traumesideleie, gjerne i vakuummadrass!
… og skal du transportere meg bevisstløs: Bruk Traumesideleie, gjerne i vakuummadrass!

43
?

Liknende presentasjoner

















 litt om trinnene…….>")

