Laste ned presentasjonen
Presentasjon lastes. Vennligst vent

1
Dosering av trombocytt- og erytrocyttkonsentrater- tid for nytenkning ?
Tor Hervig Avdeling for immunologi og transfusjonsmedisin, Haukeland universitetssykehus

2
Disposisjon Innledning Dosering av trombocyttkonsentrater
Dosering av erytrocyttkonsentrater Oppsummering (Ola var fra Sandefjord: “Det gikk på engelsk og norsk, engelsk og norsk)
")
3
Vi vil hjelpe pasientene!
Hva er et trombocyttkonsentrat? Hva er et erytrocyttkonsentrat? Hva er en pasient? Til barn: Dosering ml/kg, men en enhet SAG-erytrocyttkonsentrat kan ha 40-70g hemoglobin

4
Hva trenger pasientene ?
Erytrocyttkonsentrat Oksygen til vevene Celler til å presse trombocyttene mot karveggen Hva er ønsket hb etter transfusjon? Trombocyttkonsentrat Stoppe blødning Forhindre blødning

5
Trombocyttransfusjoner
Profylaktisk transfusjon? “On demand” transfusjon? To store randomiserte studier pågår Andreas Greinacher, personlig meddelelse

6
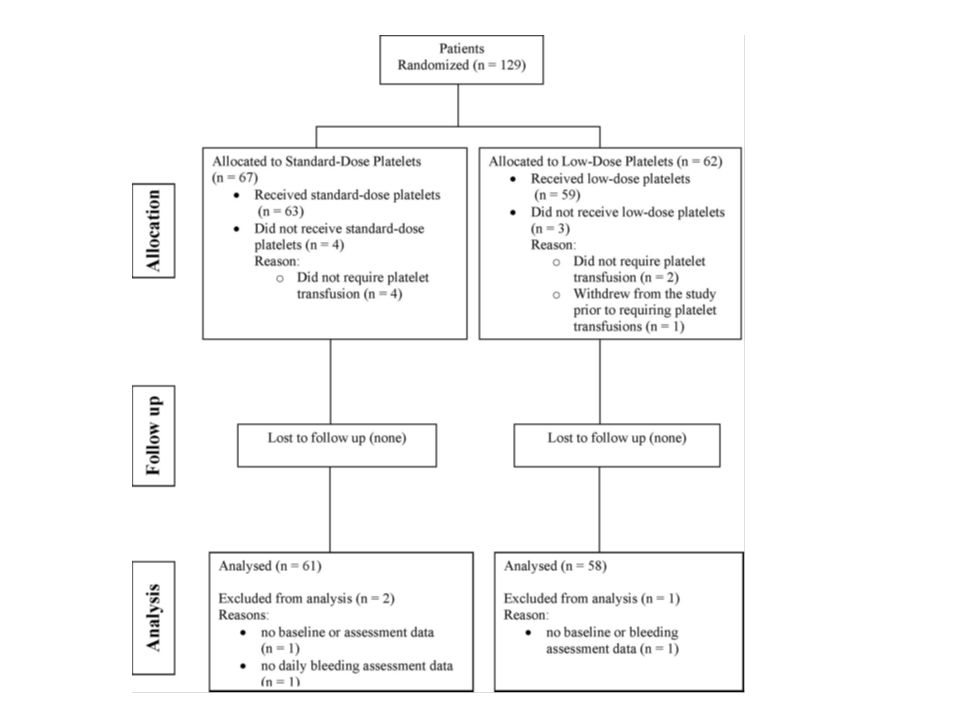
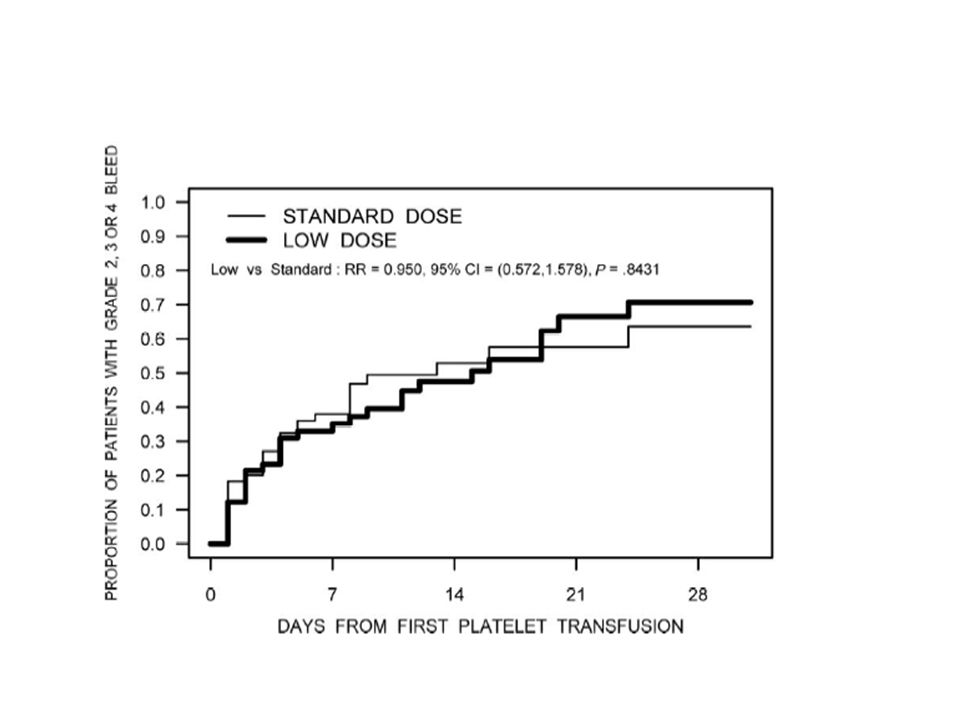
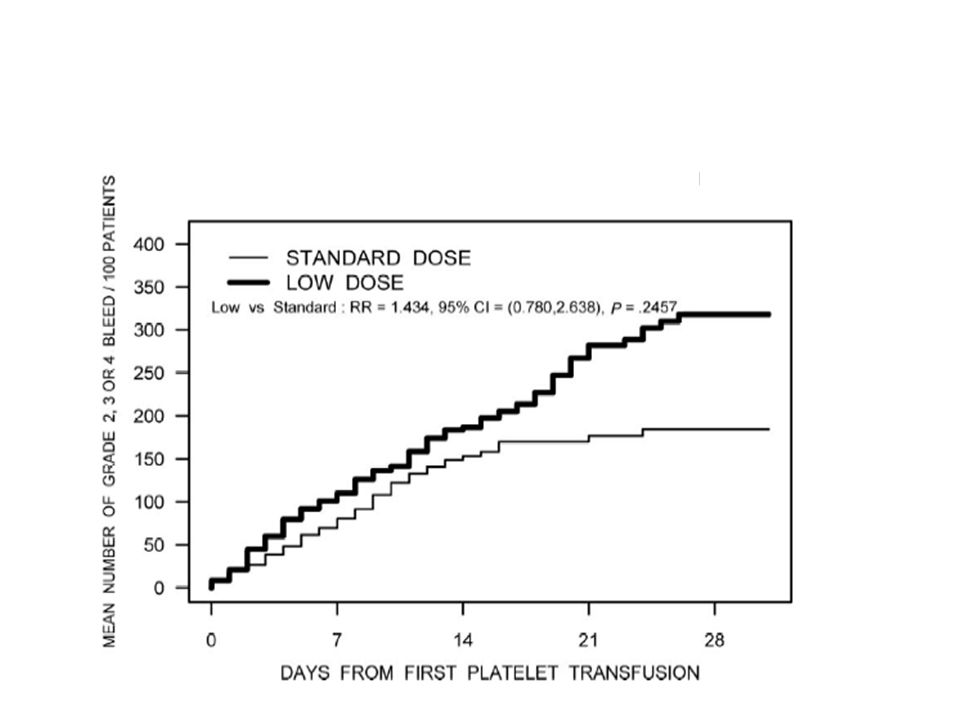
A randomized controlled trial comparing standard- and low-dose strategies for transfusion of platelets (SToP) to patients with thrombocytopenia Nancy M. Heddle, Richard J. Cook, Alan Tinmouth, C. Tom Kouroukis, Tor Hervig, Ellen Klapper, Joseph M. Brandwein, Zbigniew M. Szczepiorkowski, James P. AuBuchon, Rebecca L. Barty, and Ker-Ai Lee, for the SToP Study investigators of the BEST Collaborative Blood, 2009

7
Platedose Lav: 2,4 x 1011 Middels/standard: 4,8 x 1011 Høy: 7,2 x 1011

8
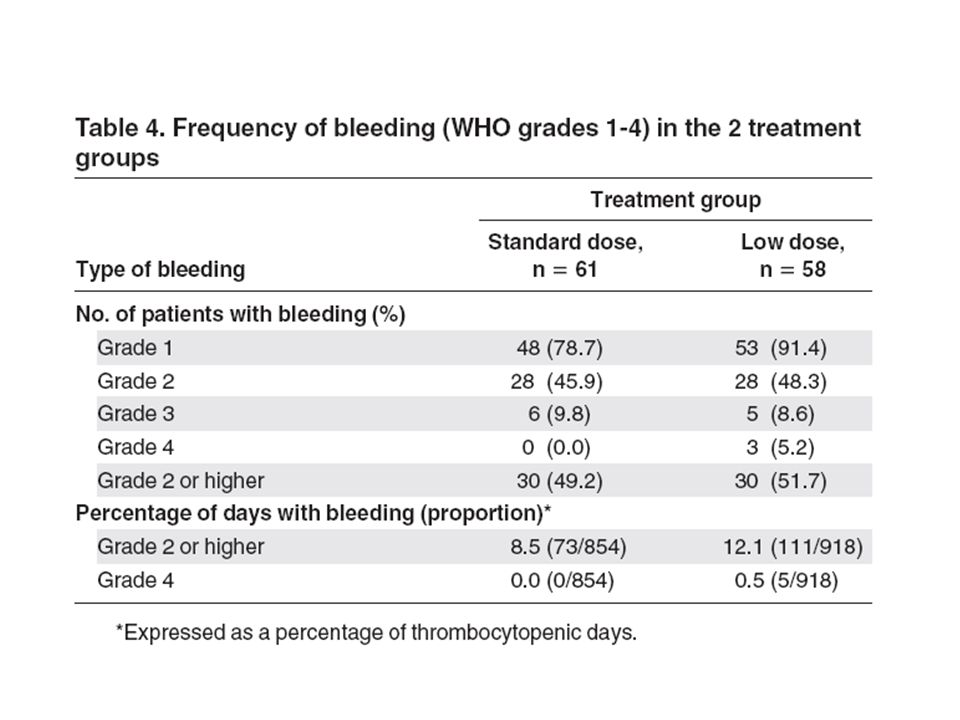
WHO blødningsskala Grad 1: Hudblødning, kortvarig neseblødning
Grad 2: Hematom, langvarig neseblødning, melena, hematemese, blødning fra stikksted (trenger ikke transfusjon) Grad 3: Som grad 2, men trenger transfusjon Grad 4: Livstruende/dødelig blødning
 Grad 3: Som grad 2, men trenger transfusjon. Grad 4: Livstruende/dødelig blødning.")
16
Mye større, amerikansk, trearmet studie
Sherril Sclichter et al: Foreløpige data: Ingen significant forskjell mellom blødningsfrekvens hos pasienter i de tre armene

17
Foreløpig konklusjon Ikke grunnlag for å endre norsk praksis
Transfusjon ved blødning???

18
OPTIMIZING STANDARDS FOR TRANSFUSION OF RED BLOOD CELL CONCENTRATE
Håkon Reikvam and Tor Hervig Haukeland University hospital and University of Bergen, Norway Chris Prowse, Products and Components R&D Group, National Science Laboratory, SNBTS, Edinburgh, UK Nancy M. Heddle, Department of Medicine, McMaster University, Hamilton, ON, Canada

19
OPTIMIZING STANDARDS FOR TRANSFUSION OF RED BLOOD CELL CONCENTRATE
An important approach to the goal of reducing number of transfusions, is to give each patient the most exact hemoglobin (Hb) dosage which is needed to achieve the wanted post-transfusion Hb.
 dosage which is needed to achieve the wanted post-transfusion Hb.")
20
The rule of thumb used in the clinical practice:
1 unit of red blood cells transfused to an adult increases hemoglobin concentration with 1 g/dl

21
Unfortunately, the Hb content of the units does not represent a homogeneity.
The blood volumes of the patients vary significantly

22
Today situation

23
Ideal situation

24
Methods Two different concepts are proposed to overcome this challenges: Standardize the units. Adjust the Hb dose according to the patient’s blood volume; Hemoglobin dosing.

25
STANDARIZATION OF THE UNITS
The term “unit” is derived from the time when “one unit of whole blood” referred to the source, i.e. a whole blood donation

26
Standardization of the red cell product
The advantage of a standardized red cell product lies in the greater degree of predictability of clinical outcome for any predefined recipient. This could result in an alteration in physician’s prescribing practices, avoiding over-transfusion, especially in low volume recipients. The current situation where red cell products are prescribed in non-standard 'units' is outdated and unscientific. Sweeney JD: Standardization of the red cell product. Transfus Apher Sci 2006, 34(2):
:")
27
Hemoglobin dosing As high as a 50-percent difference in Hb content can be encountered between two units (40-60g) Indicating that RBC transfusions should be based on Hb content of the products instead of units. Gorlin J, Cable R: What is a unit? Transfusion 2000, 40:

28
Matching the Hb dose to the individual needs of the patients reduced the total usage of red cell concentrates by approximately 30 % in a study from Turkey. Calculating the patients’ total need of Hb to achieve the targeted Hb made this possibly. The total amount of transfused RBCc was reduced to 72 from the original 104 units required (ca 30%). The success rate was closely linked to patients’ weight; increased weight correlated with failure to comply with the goal. Arslan O, Toprak S, Arat M, Kayalak Y: Hb content-based transfusion policy successfully reduces the number of RBC units transfused. Transfusion 2004, 44(4):
. The success rate was closely linked to patients’ weight; increased weight correlated with failure to comply with the goal. Arslan O, Toprak S, Arat M, Kayalak Y: Hb content-based transfusion policy successfully reduces the number of RBC units transfused. Transfusion 2004, 44(4):")
29
Pilot study Bergen, Norway Hamilton, Canada Edinburgh, UK

30
Pilot study Hemodynamically stable patients needing “pop-up” transfusions Measure hemoglobin content in red cell concentrates Measure height and weight of patients -> calculate blood volume Record pre- and post transfusion hemoglobin concentration

31
Goals To evaluate feasibility (practicability) of such procedures
To evaluate if there is correlation between hemoglobin transfused and hemoglobin increment in patients – per litre of estimated blood volume

32
Body surface (BSA) Body surface was calculated by method described by DuBois BSA (m2) = Weight (kg)0.425 x Height (cm)0.725 x
 = Weight (kg)0.425 x Height (cm)0.725 x")
33
Blood volume – alternative (BV)
Males BSA x Females BSA x

34
50 patients were included in the study
Total number of 52 transfusions episodes: -27 for women, 25 for men

36
114 units

37
Resultater Videre resultater kan ikke legges ut pga rettigheter til artikkel under vurdering. Det var signifikant samnmenheng mellom hb dose gitt og hb stigning korrigert for kroppsvolum. Dette gir grunnlag for videre arbeid.

38
Discussion Feasibility
Hemoglobin measurements were not causing a lot of extra work In the laboratory: Sterile docking of sample bag; transfer to test tube, hemoglobin measurement

39
Simplification By just measuring the weight of each unit, correlation and calculation of the actually Hb content in each unit can easily be done.

40
Allow the blood banks to use high-Hb-content units rationally by using an in-house blood-banking software. Adopting a policy of transfusing RBC in single-unit, instead of the standard two units. Alter the physicians prescribing practice and stimulate to increased cooperation with the blood bank. Avoiding potential both over-transfusion (in low weight patient) and under-transfusion (in high weight patient). Potential of reducing iron overload for patients depending on multiple transfusions.
 and under-transfusion (in high weight patient). Potential of reducing iron overload for patients depending on multiple transfusions.")
41
By just measuring the weight of each unit, correlation and calculation of the actually Hb content in each unit can easily be done.

42
How to go on? Planning a large randomized study on hemoglobin increment after red cell transfusion in Bergen (NORWAY?) Using the method of : Targeting hemoglobin concentration after transfusion. Measuring the weight of each unit

43
That about qualitative aspects?

44
Koch CG, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med. 2008;358:

45
Take home message Hemoglobin content in the units show great variability Blood volume in patients vary as well A hemoglobin increment lower than expectant does not necessary indicate active loss (bleeding, hemolytic reaction, etc.) Future aspects of more standardized procedures.
 Future aspects of more standardized procedures.")
46
Hva skal vi gjøre? Tenke oss om
Samtale med kliniske leger (og pasienter?) Gjennomføre en større studie med samme design? Ny, randomisert studie: Tilfeldige SAG mot utvalgte SAG? Hvem vil være med?
 Gjennomføre en større studie med samme design Ny, randomisert studie: Tilfeldige SAG mot utvalgte SAG Hvem vil være med")
47
Oppsummering Platedose har neppe betydning for utfall hos pasienten
Vi venter i spenning på kunnskap om forebyggende versus terapeutiske trombocyttransfusjoner Erytrocyttransfusjoner basert på “enhetstanken” gir vilkårlige konsekvenser for pasientene, på en eller annen måte må vi forbedre praksis: Til beste for pasient og blodbeholdning

Liknende presentasjoner














 Bjart Holtsmark (SSB) Ole Røgeberg (Frisch)>")






